Image Type
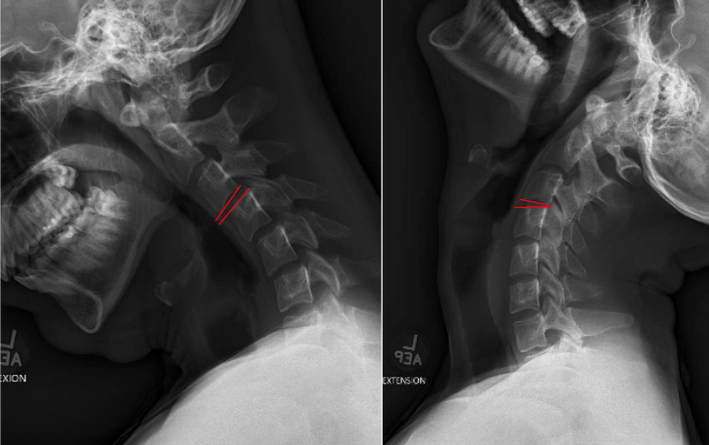
Cervical Flexion-Extension
1) Description of Measurement
Cervical angulation, also referred to as segmental rotation, measures the change in angular alignment between two adjacent vertebrae when the neck moves from full flexion to full extension.
This dynamic parameter assesses ligamentous integrity, facet stability, and functional motion in the subaxial cervical spine (C2–C7). Excessive angulation reflects segmental instability, commonly arising from trauma, degenerative disc disease, facet insufficiency, or postoperative complications.
The measurement focuses on the angular difference between vertebral endplates at each functional motion segment.
This is measuring total range of motion at each segment, which is distinct from the White-Panjabi criterion for angular discontinuity between adjacent segments.
2) Instructions to Measure
Obtain Lateral Flexion and Extension X-rays
Ensure full functional flexion and extension without patient guarding.
Visualize vertebrae C2 through C7 clearly in both views.
Select the Motion Segment
Typically measured at C2–C3 through C6–C7.
Identify the superior endplate of the inferior vertebra and the inferior endplate of the superior vertebra for each motion segment.
Draw Measurement Lines
For each segment on flexion and extension films:Draw a straight line along the inferior endplate of the superior vertebra (e.g., C4).
Draw a straight line along the superior endplate of the adjacent inferior vertebra (e.g., C5).
Measure the Angle in Each Position
Use PACS angle tools to measure the intervertebral angle in flexion and extension.
Angles typically open posteriorly in extension and anteriorly in flexion.
Calculate Segmental Angulation
Angulation = |Angle in Flexion − Angle in Extension|
Record the angulation for each segment (C2–C3 through C6–C7).
Interpret Maximum Instability
The segment with the largest motion is typically reported as the key instability level.
3) Normal vs. Pathologic Ranges
Normal segmental motion (flexion to extension):
C2-C3: approximately 11-12°
C3-C4: approximately 12-15°
C4-C5: approximately 15-19°
C5-C6: approximately 19-20°
C6-C7: approximately 20°
Pathologic patterns suggesting instability:
Segmental hypermobility: Motion significantly exceeding normal ranges for that level (e.g., >20-25° at mid-cervical levels)
Angular discontinuity (White-Panjabi criterion): >11° difference in angulation between adjacent segments on a single lateral view, indicating focal kinking or curvature discontinuity
Focal hypermobility: One segment demonstrating markedly greater motion than adjacent levels, suggesting localized ligamentous or facet failure
Key distinction: The 11° White-Panjabi criterion measures angular difference between adjacent vertebrae on a single radiograph (capturing segmental kinking), not the total range of motion between flexion and extension.
4) Important References
White AA, Panjabi MM. Clinical Biomechanics of the Spine. 2nd ed. Lippincott Williams & Wilkins; 1990.
Dvorak J, Panjabi MM. Functional anatomy, injury, and instability of the cervical spine. Spine. 1987;12(8):831–837.
Harris JH Jr, Edeiken-Monroe B. The Radiology of Emergency Medicine. Williams & Wilkins; 1993.
Tang B, Yao H, Wang S, et al. In vivo 3-dimensional kinematics study of the healthy cervical spine based on CBCT combined with 3d-3d registration technology. Spine (Phila Pa 1976). 2021;46(24):E1301-E1310.
Muhle C, Wiskirchen J, Weinert D, et al. Biomechanical aspects of the subarachnoid space and cervical cord in healthy individuals examined with kinematic magnetic resonance imaging. Spine (Phila Pa 1976). 1998;23(5):556-567.
Knight RQ. Complementary angles. A simplification of sagittal plane rotational assessment in cervical instability. Spine (Phila Pa 1976). 1993;18(6):755-758.
5) Other info....
Angulation measurement complements C2–C7 translation, providing both rotational and translational assessments of stability.
Excess angulation typically indicates compromise of:
Facet capsules
Posterior ligamentous complex
Intervertebral disc
Flexion–extension views must not be performed until fracture or dislocation is excluded via CT.
Dynamic instability often becomes apparent only in flexion–extension films, even when neutral films appear stable.
Segmental angulation is especially useful in:
Trauma evaluation
Whiplash-associated disorders
Postoperative fusion assessment
Adjacent segment degeneration
Use calibrated PACS tools to improve accuracy and minimize parallax errors.