Image Type
Sagittal Canal Diameter
1) Description of Measurement
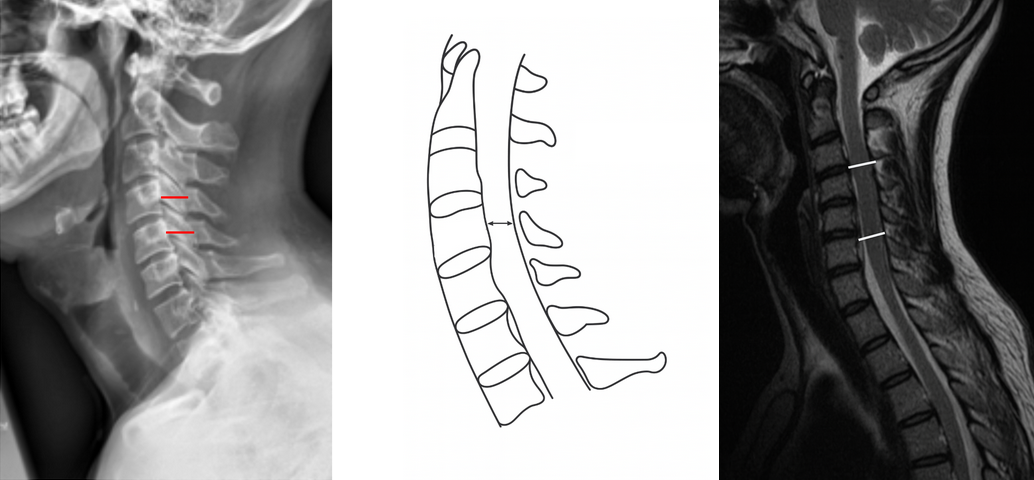
The Sagittal Canal Diameter (also known as the anteroposterior canal diameter) is a direct radiographic measurement of the bony spinal canal on a lateral cervical spine X-ray.
It assesses the anteroposterior (AP) dimension of the spinal canal, which is crucial for detecting cervical canal stenosis, whether congenital or acquired.
A reduced sagittal canal diameter correlates with spinal cord compression, myelopathy, and increased vulnerability to cord injury even after minor trauma.
This measurement is often complemented by the Pavlov/Torg Canal-to-Body Ratio, which normalizes for radiographic magnification and vertebral size.
2) Instructions to Measure
Obtain a neutral lateral cervical spine X-ray (as shown in the attached images).
Select the vertebral level to assess (typically C3–C7).
Identify two landmarks at the chosen level:
Posterior surface of the vertebral body (anterior canal boundary).
Spinolaminar line (posterior canal boundary).
Measure the shortest perpendicular distance between these two points — from the posterior vertebral body to the inner margin of the spinolaminar line.
This measurement represents the sagittal diameter of the canal (in millimeters).
Repeat for multiple levels (C3–C7) and record the smallest value, as this indicates the narrowest portion of the canal.
Ensure the X-ray is properly centered and the head is neutral to avoid magnification errors or projectional distortion.
3) Normal vs. Pathologic Ranges
Normal canal diameter (C3-C7): ≥ 13 mm
Relative stenosis (C3-C7): < 13 mm; increased risk of cord compression/myelopathy
Absolute stenosis (C3-C7): < 10 mm; high risk of cord compression/myelopathy
Normal canal diameter (C1): ~21 mm; stenosis rare at this level
Normal canal diameter (C2): ~ 20 mm; stenosis rare at this level
4) Important References
Pavlov H, Torg JS, Robie B, Jahre C. Cervical spinal stenosis: determination with vertebral body ratio method. Radiology. 1987;164(3):771–775.
Hinck VC, Sachdev NS. Developmental stenosis of the cervical spinal canal. Brain. 1966;89(1):27–36.
Morishita Y, Naito M, Hymanson HJ, et al. The relationship between the Torg–Pavlov ratio and spinal cord area in the cervical spine: a study using MRI. Spine. 2009;34(5):E197–E202.
Torg JS, Pavlov H, Genuario SE, et al. Neck injuries to athletes: a prospective study of the cervical spinal canal. J Bone Joint Surg Am. 1986;68(9):1354–1363.
5) Other info....
Direct measurement of sagittal canal diameter provides an absolute canal size but may vary with X-ray magnification; hence, many clinicians prefer the Pavlov/Torg Ratio as a normalized index.
MRI is the gold standard for assessing true spinal canal dimensions and cord compression, as it visualizes both bony and soft tissue structures.
CT is most accurate for bony canal assessment, particularly for evaluating congenital stenosis or ossification of the posterior longitudinal ligament (OPLL).
Dynamic flexion-extension X-rays can reveal positional narrowing in cases of ligamentous instability or spondylotic stenosis.
The C5–C6 level most commonly exhibits the smallest canal and is often the first site of symptomatic stenosis.
Congenital stenosis is defined by uniformly narrow canals, whereas acquired stenosis is usually segmental and associated with degenerative changes (osteophytes, disc protrusion).