Image Type
Occipital Condyle–C1 Interval (CCI)
1) Description of Measurement
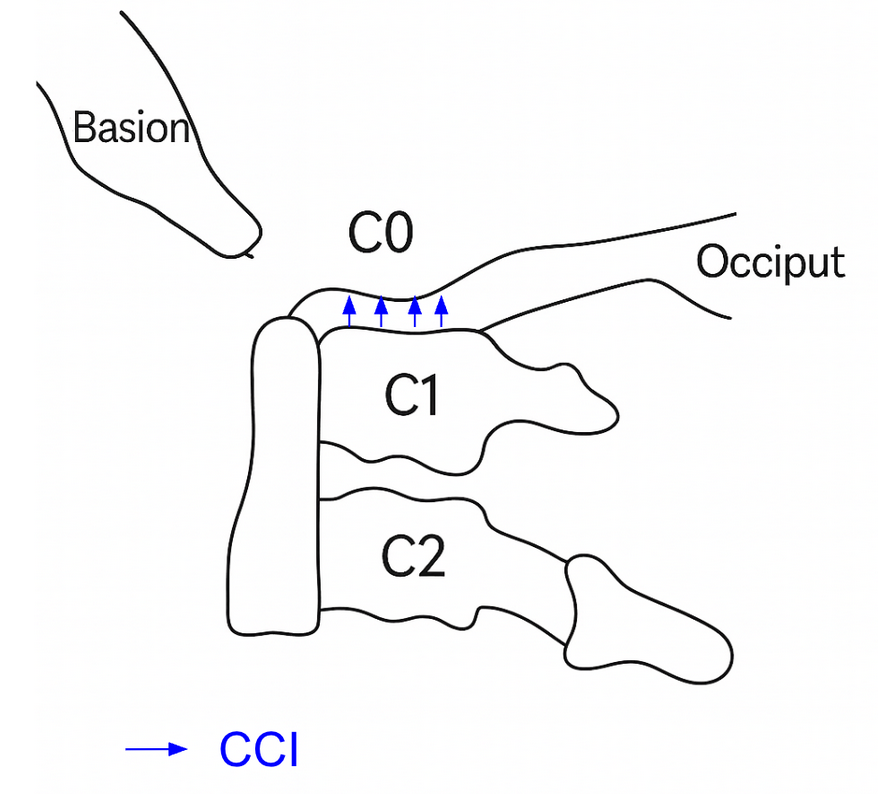
The Occipital Condyle–C1 Interval (CCI) is a radiographic measure of atlanto-occipital joint stability. It evaluates for symmetry and widening by measuring the distance between the occipital condyles and the superior articular surface of the lateral masses of C1 (atlas) on each side in sagittal and coronal views.
An increased interval reflects disruption of the tectorial membrane, alar ligaments, or joint capsule, consistent with atlanto-occipital dislocation (AOD).
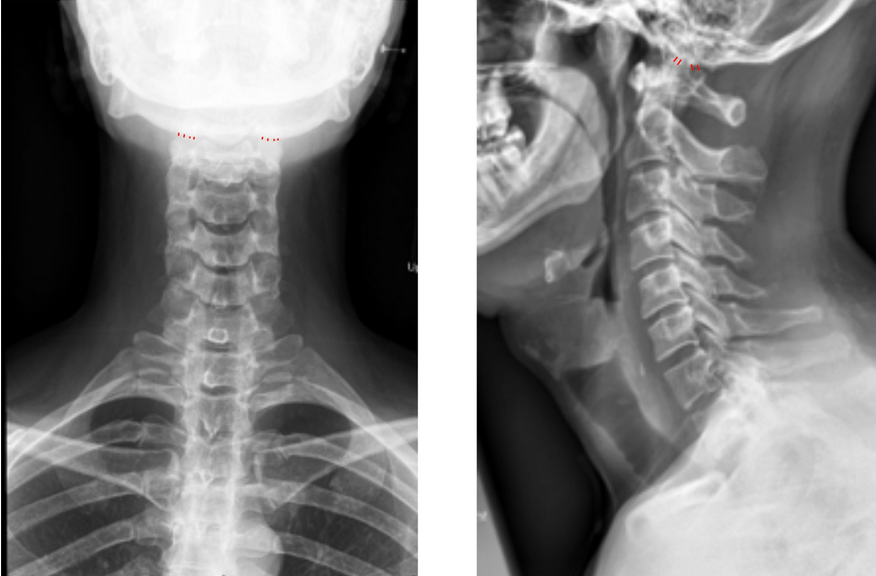
While originally measured on CT, CCI can also be estimated on well-positioned AP open-mouth or lateral cervical X-rays as a screening tool when CT is unavailable.
2) Instructions to Measure
Obtain both AP open-mouth odontoid and lateral cervical spine X-rays (as shown in the provided images).
Identify landmarks on each side:
Occipital condyle: The inferior articular surface of the occipital bone where it articulates with C1.
Superior articular surface of C1 (atlas lateral mass): The concave superior facet just below the occipital condyle.
On each side, measure the shortest perpendicular distance between the inferior margin of the occipital condyle and the superior margin of the C1 lateral mass.
Record both the right and left CCI values and calculate the average.
On lateral view, identify the posterior margins of the condyle and atlas and measure the shortest perpendicular distance between the inferior margin of the occipital condyle and the superior margin of the C1 lateral mass.
Repeat the process on the contralateral side
3) Normal vs. Pathologic Ranges
Normal CCI (adults): ≤ 2 mm (symmetric)
Pathologic CCI (adults): > 4 mm (or asymmetry > 2 mm); suggestive of AOD
Normal CCI (children): ≤ 5 mm (increased ligamentous laxity in children)
Pathologic CCI (children): > 5 mm or marked asymmetry between sides; suggestive of AOD
A mean CCI > 1.5 mm or asymmetry > 2 mm strongly correlates with atlanto-occipital dislocation, even in the absence of translation on lateral view.
4) Important References
Pang D, Nemzek WR, Zovickian J. Atlanto-occipital dislocation: Part 2—The clinical use of the occipital condyle–C1 interval. Neurosurgery. 2007;61(5):995–1014.
Harris JH Jr, Carson GC, Wagner LK, Kerr N. Radiologic diagnosis of traumatic occipitovertebral dissociation: 1. Normal occipitovertebral relationships on lateral radiographs of adults. AJR Am J Roentgenol. 1994;162(4):881–886.
Traynelis VC, Marano GD, Dunker RO, Kaufman HH. Traumatic atlanto-occipital dislocation: case report and review of the literature. Neurosurgery. 1986;19(1):112–117.
Smoker WRK. Craniovertebral junction: normal anatomy, craniometry, and congenital anomalies. Radiographics. 1994;14(2):255–277.
5) Other info....
CCI is one of the most sensitive and specific measurements for diagnosing AOD, particularly in pediatric trauma.
On X-ray, visualization can be limited, CT with coronal reconstruction is the gold standard.
When measured on X-ray, ensure the head is in a neutral position and not rotated or tilted, as asymmetry can mimic abnormal widening.
MRI complements this measurement by showing ligamentous injury or tectorial membrane disruption.
In trauma evaluation, CCI, BDI, BAI, and Power’s ratio should be assessed together for a comprehensive craniocervical junction assessment.
CCI > 4 mm on X-ray warrants immediate cervical immobilization and CT confirmation.