Image Type
Basion-Axial Interval
1) Description of Measurement
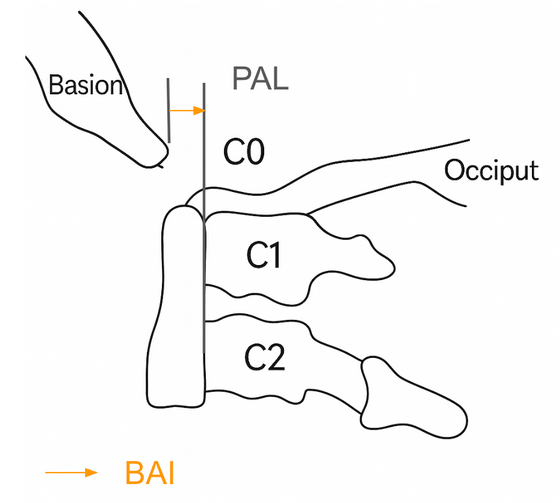
The Basion-Axial Interval (BAI), also known as the basion-posterior axial line distance, is a key radiographic measurement used to evaluate atlanto-occipital alignment and craniovertebral junction stability.
It measures the horizontal distance between the basion (the anterior margin of the foramen magnum) and a vertical line drawn along the posterior cortex of the dens (odontoid process) or posterior axial line.
This interval is particularly useful in detecting anterior or posterior translation of the occiput relative to the cervical spine, such as in atlanto-occipital dislocation (AOD) following trauma.
2) Instructions to Measure
Obtain a neutral lateral cervical spine X-ray (as shown in the attached image).
Identify the following anatomical landmarks:
Basion (B): The most anterior inferior margin of the foramen magnum.
Posterior axial line (A’): A vertical line drawn along the posterior cortex of the odontoid process (dens) and extending inferiorly along the posterior surface of the body of C2 (axis).
Measure the horizontal (anterior–posterior) distance between the basion (B) and the posterior axial line (A’).
The measurement should be taken perpendicular to the posterior axial line, not along the skull base.
Positive values indicate the basion lies anterior to the posterior axial line; negative values indicate the basion lies posterior to it.
This measurement can also be performed on CT for improved precision, particularly when the X-ray landmarks are indistinct
3) Normal vs. Pathologic Ranges
Normal BAI (adults): -4 mm to +12 mm
Pathologic/Unstable BAI (adults): > +12 mm = anterior displacement (AOD); < -4 mm = posterior displacement
Normal BAI (children): - 4mm to + 12 mm
Pathologic/Unstable BAI (children): > +12 mm, < -4 mm suggest ligamentous injury or instability
4) Important References
Harris JH Jr, Carson GC, Wagner LK, Kerr N. Radiologic diagnosis of traumatic occipitovertebral dissociation: 1. Normal occipitovertebral relationships on lateral radiographs of adults. AJR Am J Roentgenol. 1994;162(4):881–886.
Powers B, Miller MD, Kramer RS, Martinez S, Gehweiler JA Jr. Traumatic anterior atlanto-occipital dislocation. Neurosurgery. 1979;4(1):12–17.
Traynelis VC, Marano GD, Dunker RO, Kaufman HH. Traumatic atlanto-occipital dislocation: case report and review of the literature. Neurosurgery. 1986;19(1):112–117.
Smoker WRK. Craniovertebral junction: normal anatomy, craniometry, and congenital anomalies. Radiographics. 1994;14(2):255–277.
5) Other info....
The BAI is often measured together with the Basion-Dens Interval (BDI) and Power’s Ratio for comprehensive evaluation of craniovertebral stability.
On CT or MRI, the same measurement principles apply, but the posterior axial line is drawn along the posterior dens and body of C2.
In acute trauma, a widened BAI (> 12 mm) indicates tectorial membrane and alar ligament disruption—a hallmark of atlanto-occipital dislocation, which requires immediate stabilization.
The Harris Method (using both BAI and BDI) is a reliable screening tool for occipitocervical dissociation.
Ensure neutral patient head positioning; hyperflexion or hyperextension can artificially alter the measurement.