
Image Type
Basion-Dens Interval (BDI)
1) Description of Measurement
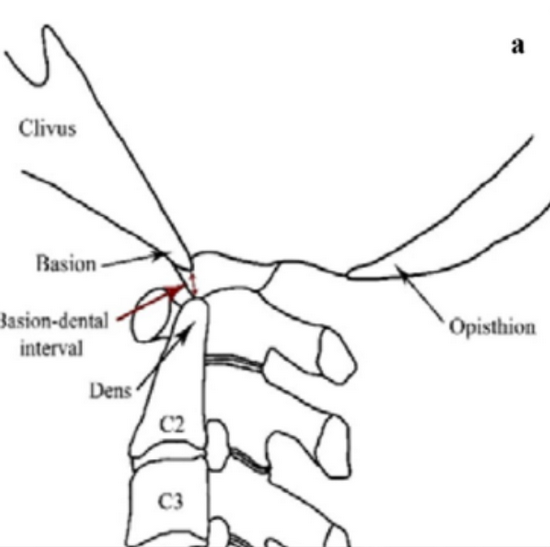
The Basion-Dens Interval (BDI) is a radiographic measurement used to assess atlanto-occipital alignment and integrity of the craniovertebral junction.
It measures the distance between the basion (anterior margin of the foramen magnum) and the tip (apex) of the odontoid process (dens).
An increased BDI indicates potential atlanto-occipital dislocation (AOD) or craniovertebral instability — conditions often seen in high-energy trauma, rheumatoid arthritis, or congenital ligamentous laxity.
2) Instructions to Measure
Obtain a neutral lateral cervical spine X-ray (as shown in the provided images).
Identify the following landmarks:
Basion (B): The anterior inferior margin of the foramen magnum (visible as the anterior skull base point).
Tip of the Dens (D): The most superior point of the odontoid process (C2).
Draw a straight line from the basion (B) to the tip of the dens (D).
Measure the shortest linear distance between these two points — this is the BDI.
The measurement should be taken perpendicular to the cranial base, not along the dens axis.
For suspected instability, repeat on flexion and extension views (if clinically indicated/safe).
3) Normal vs. Pathologic Ranges
Normal BDI (adults): ≤ 12 mm
Pathologic BDI (adults): > 12 mm; suggests atlanto-occipital dissociation
Normal BDI (children): ≤ 10 mm
Pathologic BDI (children): > 10 mm; may indicate instability due to ligamentous laxity
4) Important References
Harris JH Jr, Carson GC, Wagner LK, Kerr N. Radiologic diagnosis of traumatic occipitovertebral dissociation: 1. Normal occipitovertebral relationships on lateral radiographs of adults. AJR Am J Roentgenol. 1994;162(4):881–886.
Powers B, Miller MD, Kramer RS, Martinez S, Gehweiler JA Jr. Traumatic anterior atlanto-occipital dislocation. Neurosurgery. 1979;4(1):12–17.
Traynelis VC, Marano GD, Dunker RO, Kaufman HH. Traumatic atlanto-occipital dislocation: case report and review of the literature. Neurosurgery. 1986;19(1):112–117.
Smoker WRK. Craniovertebral junction: normal anatomy, craniometry, and congenital anomalies. Radiographics. 1994;14(2):255–277.
5) Other info....
The BDI is often evaluated alongside Power’s Ratio, Basion-Axial Interval (BAI), and Atlanto-Dental Interval (ADI) for a complete assessment of occipitocervical stability.
CT is the gold standard for confirming measurements and detecting subtle dislocations, while MRI is used to assess ligamentous injury.
A BDI > 12 mm in adults (or > 10 mm in children) strongly indicates disruption of the tectorial membrane or alar ligaments, which normally tether the occiput to the dens. In trauma settings, this often requires immobilization and surgical stabilization.
Pediatric patients may have physiologic widening due to ligamentous elasticity — correlation with clinical findings is essential.
Always ensure neutral positioning; flexion or extension can artifactually increase or decrease the interval.

Nicholson LL, Rao PJ, Lee M, Wong TM, Cheng RH, Chan C. Reference values of four measures of craniocervical stability using upright dynamic magnetic resonance imaging. La radiologia medica. 2023 Mar;128(3):330-9.