
Image Type
Facet Joint Overlap (Percent Overlap Method)
1) Description of Measurement
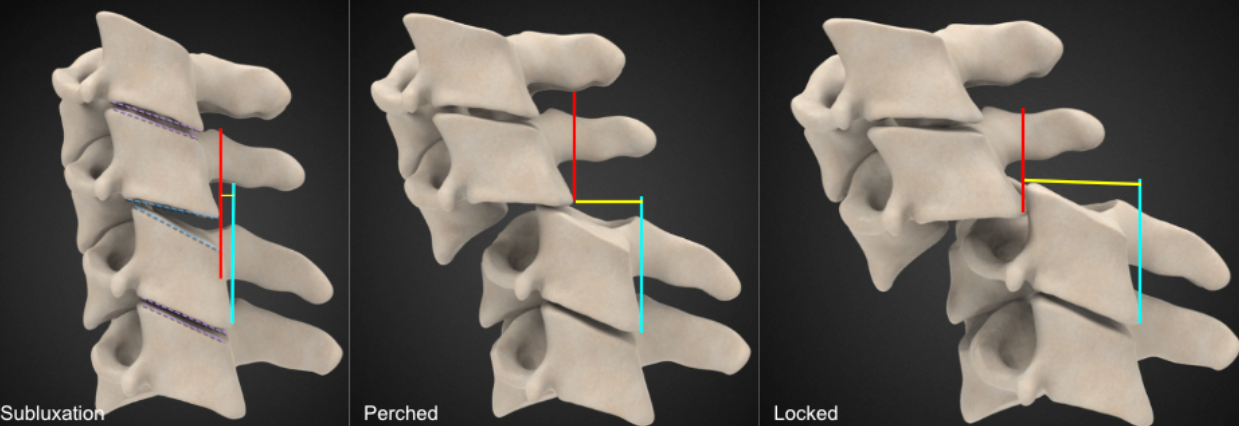
Facet joint step-off quantifies the anteroposterior displacement between articulating cervical facet joints and is used to identify facet subluxation, perched facets, and locked (jumped) facets, which represent progressively severe forms of posterior element instability.
This measurement assesses the degree of malalignment between the inferior articular facet of the superior vertebra and the superior articular facet of the inferior vertebra. Increasing step-off distance reflects escalating mechanical instability and is strongly associated with disco-ligamentous injury, neurologic risk, and the need for surgical stabilization.
2) Instructions to Measure
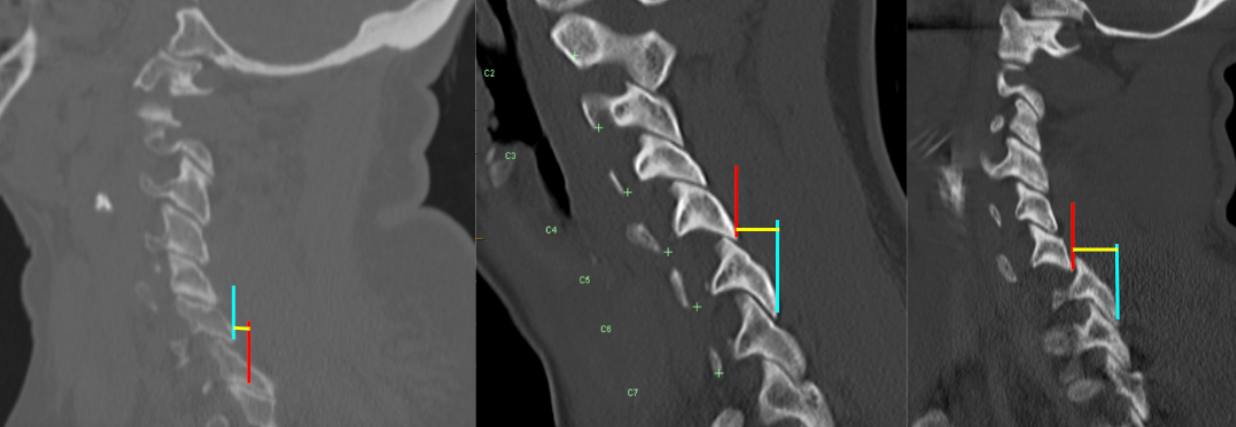
Obtain thin-slice cervical CT with sagittal and oblique reconstructions optimized to visualize the facet joints.
Identify the facet level of interest, particularly where abnormal alignment is suspected.
On the selected slice:
Identify the posterior margin of the inferior articular facet of the superior vertebra.
Identify the posterior margin of the superior articular facet of the inferior vertebra.
Draw two vertical reference lines along these posterior cortical margins.
Measure the horizontal anteroposterior distance (mm) between the two lines:
This distance represents the facet joint step-off.
Perform measurements bilaterally and record the largest step-off, as this represents the worst degree of instability.
3) Normal vs. Pathologic Ranges
Normal: ≤ 1 mm; intact facet articulation
Facet subluxation: 1 - 3 mm; partial displacement, potentially unstable
Perched facet: > 3 mm; inferior facet rests of superior facet; unstable
Locked (jumped) facet: complete anterior displacement; gross instability
Key points:
Perched facets represent an incomplete dislocation and are often unstable.
Locked facets indicate failure of the posterior ligamentous complex and are almost always unstable.
Findings may be unilateral or bilateral, with bilateral injuries carrying greater instability.
4) Important References
Allen BL Jr, Ferguson RL, Lehmann TR, O'Brien RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine (Phila Pa 1976). 1982 Jan-Feb;7(1):1-27. doi: 10.1097/00007632-198200710-00001.
Harris JH Jr, Mirvis SE. The Radiology of Acute Cervical Spine Trauma. 3rd ed. Williams & Wilkins; 1996.
Dvorak MF, Fisher CG, Fehlings MG, et al. The surgical approach to subaxial cervical spine injuries: an evidence-based algorithm based on the SLIC classification system. Spine (Phila Pa 1976). 2007 Nov 1;32(23):2620-9. doi: 10.1097/BRS.0b013e318158ce16.
Daffner RH, Sciulli RL, Rodriguez A, Protetch J. Imaging for evaluation of suspected cervical spine trauma: a 2-year analysis. Injury. 2006 Jul;37(7):652-8. doi: 10.1016/j.injury.2006.01.018.
5) Other info....
Facet step-off is a direct measure of mechanical instability, complementing:
Facet overlap percentage
Anterior/posterior vertebral translation
Interspinous widening
CT is the gold standard for detecting facet displacement and fractures.
MRI is recommended when step-off is identified to evaluate:
Disco-ligamentous injury
Spinal cord compression
Unilateral locked facets are commonly associated with rotational injuries.
Bilateral locked facets often result in significant canal compromise and neurologic injury.
Even small step-off distances may be clinically significant in the presence of neurologic symptoms or associated ligamentous disruption.
Adapted from: Jones J, Baba Y, Bell D, et al. Facet dislocation. Reference article, Radiopaedia.org (Accessed on 20 Dec 2025) https://doi.org/10.53347/rID-9092