
Image Type
Grabb-Oakes Measurement (pB - C2 line)
1) Description of Measurement
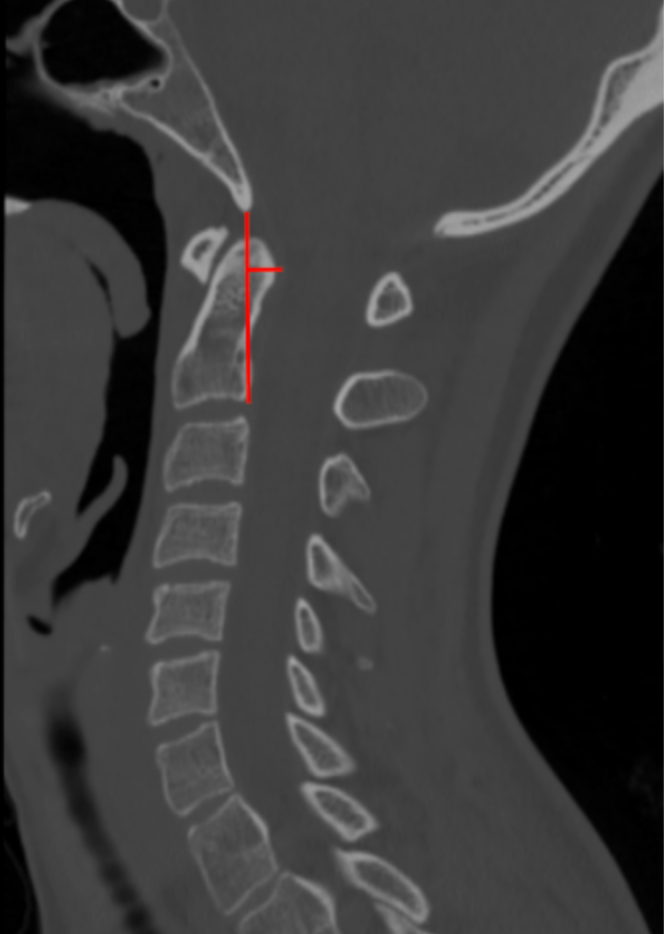
The Grabb–Oakes measurement, also referred to as the pB–C2 line, quantifies the degree of ventral brainstem compression at the craniovertebral junction. It measures the perpendicular distance from the posterior surface of the odontoid or ventral soft tissue mass to a reference line drawn between the basion and the posteroinferior aspect of the C2 vertebral body.
This measurement is especially useful in identifying clinically significant basilar invagination, retro-odontoid pseudotumor, pannus formation, and craniocervical instability, all of which may produce deformative ventral compression of the cervicomedullary junction.
2) Instructions to Measure
Select a true mid-sagittal CT reconstruction that clearly visualizes the basion, odontoid process, and C2 vertebral body.
Identify the following landmarks:
Basion (B): the midpoint of the anterior margin of the foramen magnum.
C2 point (C2): the posteroinferior corner of the C2 vertebral body.
Draw the pB–C2 reference line:
Draw a straight line connecting the basion to the posteroinferior aspect of C2.
Identify the point of maximal ventral encroachment:
Usually the posterior surface of the odontoid or associated retro-odontoid soft tissue.
Draw a perpendicular line from the pB–C2 reference line to the point of maximal ventral encroachment.
Measure this perpendicular distance in millimeters (mm).
This value is the Grabb–Oakes (pB–C2) measurement.
3) Normal vs. Pathologic Ranges
Normal: ≤ 9 mm
Pathologic (significant ventral brainstem compression): > 9 mm
Key points:
A value > 9 mm is highly suggestive of clinically relevant ventral cervicomedullary compression.
Increasing distance correlates with worsening neurologic symptoms.
4) Important References
Grabb PA, Mapstone TB, Oakes WJ. Ventral brain stem compression in pediatric and young adult patients with Chiari I malformations. Neurosurgery. 1999 Mar;44(3):520-7; discussion 527-8. doi: 10.1097/00006123-199903000-00050.
Smoker WR. Craniovertebral junction: normal anatomy, craniometry, and congenital anomalies. Radiographics. 1994 Mar;14(2):255-77. doi: 10.1148/radiographics.14.2.8190952.
Menezes AH. Craniovertebral junction anomalies: diagnosis and management. Semin Pediatr Neurol. 1997 Sep;4(3):209-23. doi: 10.1016/s1071-9091(97)80038-1.
Martin JE, Bookland M, Moote D, Cebulla C. Standardized method for the measurement of Grabb's line and clival-canal angle. J Neurosurg Pediatr. 2017 Oct;20(4):352-356. doi: 10.3171/2017.5.PEDS17181.
5) Other info....
The Grabb–Oakes measurement should be evaluated together with:
Clivo-Axial Angle (CXA)
Basion–Axial Interval (BAI)
Basion–Dens Interval (BDI)
Power’s ratio
Particularly useful in:
Basilar invagination
Retro-odontoid pseudotumor
Rheumatoid craniovertebral disease
Congenital connective tissue disorders
When pB–C2 is > 9 mm, MRI is recommended to assess:
Ventral brainstem deformation
Spinal cord signal change
Surgical realignment or decompression aimed at reducing this measurement has been associated with improvement in neurologic symptoms in appropriately selected patients.
Adapted from: Thibodeau R, Normal CT cervical spine. Case study, Radiopaedia.org (Accessed on 28 Dec 2025) https://doi.org/10.53347/rID-183532