Image Type
C2-C7 Coronal Cobb Angle
1) Description of Measurement
The C2–C7 Coronal Cobb Angle quantifies coronal (frontal plane) alignment of the cervical spine. It is used to assess cervical scoliosis or lateral deviation of the cervical spine from the vertical axis.
This measurement provides a standardized method to evaluate deformity severity and progression, particularly in cases of congenital scoliosis, degenerative changes, trauma, or postsurgical malalignment.
It is analogous to the Cobb angle used in thoracolumbar scoliosis evaluation but applied to the cervical region (C2–C7).
2) Instructions to Measure
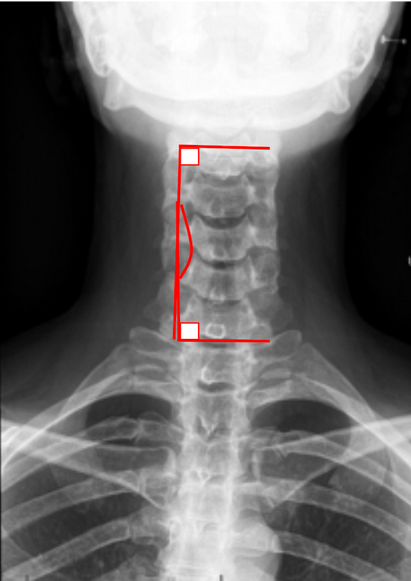
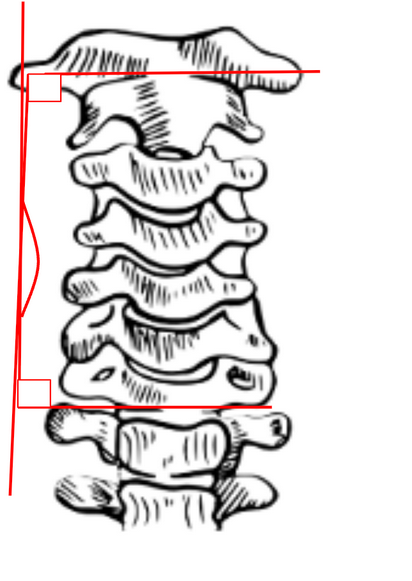
Obtain a standing anteroposterior (AP) cervical spine X-ray ensuring the patient’s head is in a neutral upright position.
Identify the superior endplate of C2 and the inferior endplate of C7.
Draw a straight line along the superior endplate of C2.
Draw another line along the inferior endplate of C7.
Construct perpendicular lines from each of these endplate lines.
The angle formed at the intersection of these perpendiculars is the C2–C7 Coronal Cobb Angle.
The angle opens toward the convexity of the deformity.
If the cervical spine deviates toward the right, it is a right-convex curve, and vice versa.
Optional:
For regional deformities (e.g., localized curves), the angle may be measured between the end vertebrae of the most tilted segments within the curve rather than fixed C2 and C7 levels.
3) Normal vs. Pathologic Ranges
Normal C2-C7 coronal alignment: < 5°
Mild C2-C7 scoliosis: 5-15°; usually asymptomatic, often postural
Moderate C2-C7 scoliosis: 15-25°; may cause asymmetric loading or muscle strain
Severe C2-C7 scoliosis: > 25°; indicates structural deformity or compensatory adaptation
4) Important References
Ames CP, Blondel B, Scheer JK, et al. Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy. Spine. 2013;38(22 Suppl 1):S149–160.
Tang JA, Scheer JK, Smith JS, et al. The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery. Neurosurgery. 2012;71(3):662–669.
Kim HJ, Lenke LG, Shaffrey CI, et al. Assessment of cervical deformity and alignment: current concepts and future directions. Spine Deform. 2015;3(6):463–472.
Lee SH, Kim KT, Seo EM, Suk KS, Kwack YH. Cervical alignment analysis in asymptomatic adults: incidence of cervical scoliosis and influence of cervical alignment parameters on coronal balance. Eur Spine J. 2014;23(4):658–667.
5) Other info....
Coronal Cobb angle > 10° is generally considered pathologic and may require serial follow-up for progression
The C2–C7 Coronal Cobb Angle is used to quantify coronal alignment and deformity in both degenerative and congenital cervical scoliosis.
Always ensure the AP view is centered and symmetric, as rotation or tilt can artifactually alter the angle.
When performing postoperative assessment, note fusion levels and any compensatory changes in the subaxial spine.
This measurement can be complemented by C7 coronal plumb line deviation (C7PL) to assess global coronal balance.
CT or EOS imaging provides higher accuracy for preoperative planning in complex deformities.