Image Type
Sagittal Vertical Axis (SVA)
1) Description of Measurement
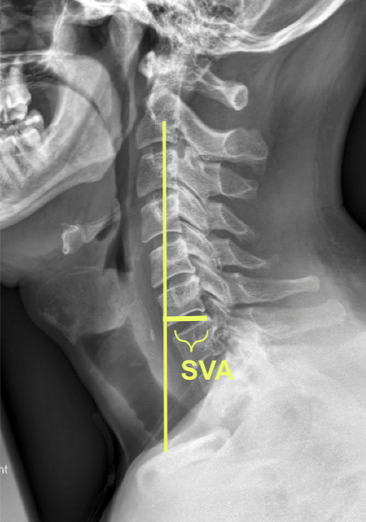
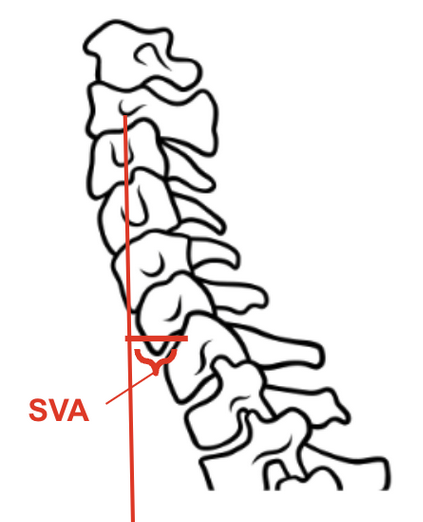
The cervical sagittal vertical axis (cSVA) is a measure of cervical sagittal alignment and global balance. It is defined as the horizontal distance (in millimeters) from the vertical plumb line dropped from the centroid of C2 to the posterior–superior corner of the C7 vertebral body on a standing lateral cervical spine x-ray.
2) Instructions to Measure
Obtain a standing lateral cervical spine x-ray with the patient looking forward in a neutral position.
Identify the C2 centroid (commonly approximated as the midpoint of the C2 vertebral body).
Drop a plumb line vertically downward from this point (parallel to the gravitational vertical).
Identify the posterior–superior corner of the C7 vertebral body.
Measure the horizontal distance between the plumb line and the posterior–superior corner of C7.
Positive value = C2 plumb line lies anterior to C7.
Negative value = C2 plumb line lies posterior to C7 (rare).
3) Normal vs. Pathologic Ranges
Normal cSVA: ~15–20 mm (range 10–20 mm in asymptomatic adults).
Pathologic: >40 mm is generally associated with positive sagittal malalignment and worse clinical outcomes (disability, pain, impaired quality of life).
Increasing cSVA reflects forward head posture / positive sagittal balance.
4) Important References
Tang JA, Scheer JK, Smith JS, et al. The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery. Neurosurgery. 2012;71(3):662–669.
Ames CP, Blondel B, Scheer JK, et al. Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy. Spine. 2013;38(22 Suppl 1):S149–160.
Smith JS, Shaffrey CI, Ames CP, et al. Assessment of cervical sagittal alignment and clinical implications. J Neurosurg Spine. 2013;19(2):141–159.
5) Other info....
Strongly correlated with Neck Disability Index (NDI): as cSVA increases, NDI worsens.
Particularly important in patients with cervical deformity (kyphosis, iatrogenic flat neck, ankylosing spondylitis).
Often reported in conjunction with cervical lordosis (C2–C7 Cobb angle) and T1 slope–cervical lordosis mismatch to better understand overall cervical alignment.