Image Type
Conus Medullaris Level and Filum Terminale Thickness (Tethered Cord)
1) Description of Measurement
Conus level refers to the lowermost tip of the spinal cord (normally around L1/L2), while filum thickness describes the fibrous strand (filum terminale) extending from it. A thickened filum (>2mm) or a low conus level (below L2/L3) often signals Tethered Cord Syndrome (TCS). It is a clinical neurological disorder caused by abnormal tissue attachments that restrict normal movement of the spinal cord within the spinal canal. This pathological fixation results in chronic traction on the spinal cord, leading to ischemia, metabolic dysfunction, and progressive neurological deterioration. While classically associated with a low-lying conus medullaris or a thickened filum terminale, tethered cord syndrome can occur even when the conus is in a normal position, particularly in adults.
2) Instructions to Measure
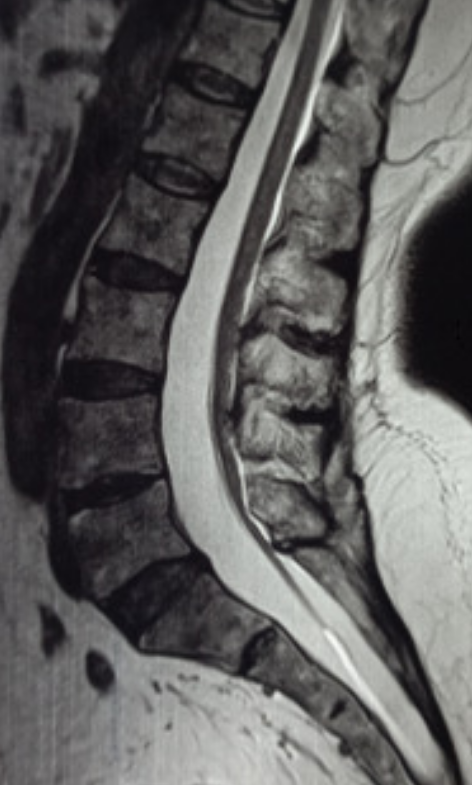
Obtain lumbosacral MRI (sagittal and axial T1/T2; include whole-spine screening when dysraphism is suspected).
Conus level
Identify the tip of the conus (transition from cord to cauda equina).
Record the vertebral level using reliable landmarks (vertebral bodies and disc spaces).
Filum thickness
Measure the filum on axial images where it is best visualized, recording its maximal diameter.
Assess for fat signal within the filum (T1 bright; fat-sat confirms).
Look for additional tethering clues that matter clinically and surgically:
Posterior displacement/taut appearance of the conus and filum
Associated lesions: filar lipoma, conus lipoma/lipomyelomeningocele, split cord malformation, dermal sinus tract, dermoid/epidermoid, arachnoid adhesions (post-op, post-trauma, infection/inflammation)
Associated skeletal findings: scoliosis, dysraphic posterior elements
Consider prone MRI when suspicion is high and supine MRI is equivocal, especially in postoperative or “occult” cases; lack of expected motion between positions can support tethering.
3) Normal vs. Pathologic Ranges
Conus position
Normal conus reaches its typical level early in life; in practice, a conus around L1–L2 is typical, and children can be slightly lower early on.
Low-lying conus is commonly defined as termination below the L2–3 disc space.
Filum terminale: Thickened filum is commonly defined as >2 mm at the L5/S1 level (most often applied in pediatric imaging; still used broadly as a practical threshold).
Fatty Filum (Filar Lipoma): Fat within the filum is seen in up to 5% of the population.
4) Important References
Hertzler DA 2nd, DePowell JJ, Stevenson CB, Mangano FT. Tethered cord syndrome: a review of the literature from embryology to adult presentation. Neurosurg Focus. 2010 Jul;29(1):E1. doi: 10.3171/2010.3.FOCUS1079. PMID: 20593997.
Agarwalla PK, Dunn IF, Scott RM, Smith ER. Tethered cord syndrome. Neurosurg Clin N Am. 2007 Jul;18(3):531-47. doi: 10.1016/j.nec.2007.04.001. PMID: 17678753.
Weisbrod LJ, Thorell W. Tethered Cord Syndrome (TCS) [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK585121/
Klekamp J. Tethered cord syndrome in adults. J Neurosurg Spine. 2011 Sep;15(3):258-70. doi: 10.3171/2011.4.SPINE10504. Epub 2011 May 20. PMID: 21599446.
5) Other info....
A meaningful subset of adult TCS can have conus at/above L2–3 and/or a filum <2 mm, so imaging alone can miss clinically tethered patients. The diagnosis should be driven by symptoms plus supportive imaging features, not measurements in isolation.