Image Type
Block Vertebra Assessment (fusion length and canal dimensions)
1) Description of Measurement
Block vertebrae are congenital anomalies resulting from failure of normal segmentation, producing fusion of two or more adjacent vertebral bodies. Assessment focuses on quantifying the length of vertebral fusion and evaluating spinal canal dimensions at and adjacent to the fused segment.
These measurements help determine the risk of adjacent segment degeneration, canal stenosis, and neurologic compromise, and are critical for preoperative planning in patients with congenital deformities or superimposed degenerative disease.
2) Instructions to Measure
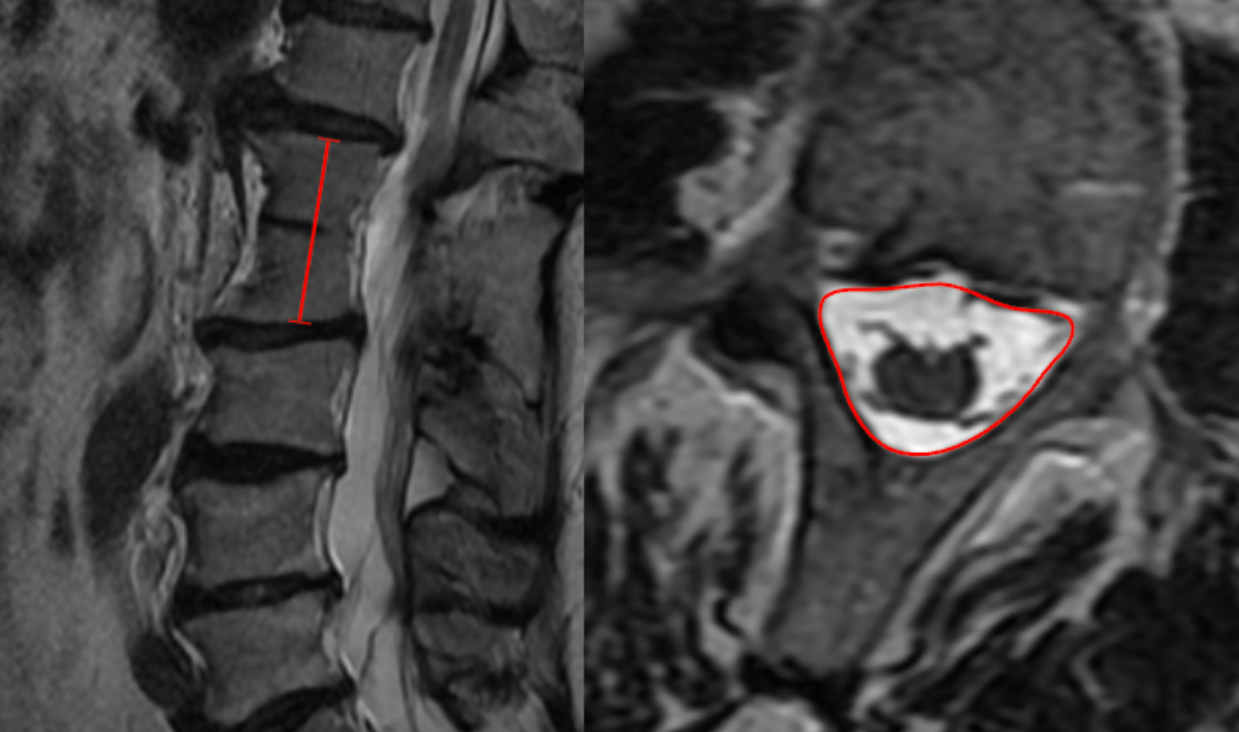
A. Fusion Length (Sagittal MRI)
Select a mid-sagittal MRI slice demonstrating the fused vertebrae.
Identify the most cranial and caudal vertebral bodies involved in the block.
Measure the craniocaudal length of the fused segment:
Draw a line from the superior endplate of the most cranial fused vertebra to the inferior endplate of the most caudal fused vertebra.
Record the distance in millimeters (mm) and note the number of fused levels.
B. Canal Dimension Assessment (Axial MRI)
Select axial T2-weighted MRI slices at:
The midpoint of the block vertebra, and
The adjacent normal levels above and below.
Measure the anteroposterior canal diameter or perform cross-sectional canal area tracing using ROI tools.
Compare canal dimensions at the fused level to adjacent levels to identify relative stenosis.
3) Normal vs. Pathologic Ranges
Isolated block: fusion length ≤ 1 vertebral level
Multilevel block (biomechanical impact): ≥ 2 levels
Moderate stenosis: canal area < 75 mm2
Severe stenosis: canal area < 50 mm2
Key points:
Longer fusion blocks increase the risk of adjacent segment disease.
Reduced canal dimensions at block levels increase risk of myelopathy.
4) Important References
Ramírez N, Cornier AS, Campbell RM Jr, Carlo S, Arroyo S, Romeu J. Natural history of thoracic insufficiency syndrome: a spondylothoracic dysplasia perspective. J Bone Joint Surg Am. 2007 Dec;89(12):2663-75. doi: 10.2106/JBJS.F.01085.
Basu PS, Elsebaie H, Noordeen MH. Congenital spinal deformity: a comprehensive assessment at presentation. Spine (Phila Pa 1976). 2002 Oct 15;27(20):2255-9. doi: 10.1097/00007632-200210150-00014.
Ma X, Du Y, Wang S, Ma J, Wang T, Kuang M, Ma B. Adjacent segment degeneration after intervertebral fusion surgery by means of cervical block vertebrae. Eur Spine J. 2018 Jun;27(6):1401-1407. doi: 10.1007/s00586-017-5371-5.
5) Other info....
Block vertebrae are commonly associated with:
Klippel–Feil syndrome
Hemivertebrae
Congenital bars
MRI is preferred for:
Identifying associated spinal cord anomalies (syringomyelia, tethered cord)
Assessing adjacent disc degeneration
Should be interpreted alongside:
Segmental mobility studies
Sagittal alignment
Documentation should include:
Number of fused levels
Exact vertebral levels involved
Canal dimensions at fused and adjacent segments