
Image Type
Presence of T1 Hypointensity (chronic myelopathy/atrophy)
1) Description of Measurement
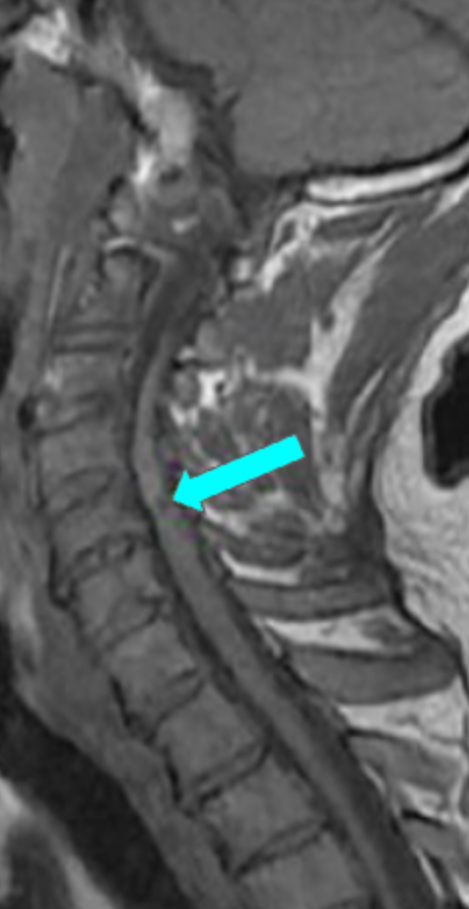
T1 hypointensity refers to focal or diffuse low signal intensity within the cervical spinal cord on T1-weighted MRI. When present, it is considered a marker of chronic spinal cord injury, most commonly representing myelomalacia, cord atrophy, gliosis, or irreversible ischemic damage.
In the context of cervical spinal stenosis or degenerative cervical myelopathy (DCM), T1 hypointensity is associated with longstanding compression, advanced disease, and poorer neurologic recovery compared with patients who demonstrate T2 hyperintensity alone.
2) Instructions to Measure
Select a mid-sagittal T1-weighted MRI sequence with adequate visualization of the cervical spinal cord.
Identify the signal intensity of normal spinal cord at levels above and below the area of interest to establish a baseline reference.
Evaluate the spinal cord at the level(s) of compression for:
Focal or linear regions of decreased T1 signal within the cord parenchyma
Signal that is clearly darker than adjacent normal cord and not attributable to artifact
Confirm that the hypointense signal:
Corresponds anatomically to the region of chronic compression
Persists across adjacent slices, when available
Record the finding as:
T1 hypointensity: Present (across multiple levels?)
T1 hypointensity: Absent
3) Normal vs. Pathologic Ranges
Normal cord signal or potentially reversible injury: No T1 hypointensity
Chronic cord injury: Focal T1 hypointensity; suggests early myelomalacia
Advanced chronic myelopathy: Diffuse or multilevel T1 hypointensity; cord atrophy
Key points:
T1 hypointensity is always pathologic
Indicates irreversible spinal cord damage in most cases
Strongly associated with poor postoperative neurologic recovery
4) Important References
Morishita Y, Naito M, Hymanson HJ, et al. The relationship between the cervical spinal canal diameter and the pathological changes in the cervical spine. Eur Spine J. 2009; Jun; 18(6):877-83.
Tetreault L, Palubiski LM, Kryshtalskyj M, et al. Significant Predictors of Outcome Following Surgery for the Treatment of Degenerative Cervical Myelopathy: A Systematic Review of the Literature. Neurosurg Clin N Am. 2018 Jan;29(1):115-127.e35.
Badhiwala JH, Wilson JR, Fehlings MG. Global burden of traumatic brain and spinal cord injury. Lancet Neurol. 2019 Jan;18(1):24-25.
Nouri A, Martin AR, Mikulis D, et al. Magnetic resonance imaging assessment of degenerative cervical myelopathy: a review of structural changes and measurement techniques. Neurosurg Focus. 2016 Jun;40(6):E5.
5) Other info....
T1 hypointensity should always be interpreted in conjunction with T2 hyperintensity:
T2 hyperintensity alone → edema or potentially reversible injury
T1 hypointensity + T2 hyperintensity → chronic, irreversible damage
Presence of T1 hypointensity is a negative prognostic factor for:
Neurologic recovery after decompression
Functional improvement (JOA, mJOA, NDI)
Absence of T1 hypointensity does not exclude clinically significant myelopathy
Particularly useful when combined with:
T2 hyperintensity length
Cord cross-sectional area (CSA)
Compression ratio
Maximum spinal cord compression (MSCC)
Adapted from: Nouri A, Martin AR, Mikulis D, Fehlings MG. Magnetic resonance imaging assessment of degenerative cervical myelopathy: a review of structural changes and measurement techniques. Neurosurg Focus. 2016 Jun;40(6):E5.