
Image Type
Compression Ratio (AP diameter transverse diameter of cord)
1) Description of Measurement
The compression ratio is a morphometric MRI parameter that quantifies the degree of cervical spinal cord deformation by comparing the anteroposterior (AP) diameter of the cord to its transverse (left–right) diameter on axial imaging.
This ratio reflects the shape distortion of the spinal cord rather than absolute size alone. A reduced compression ratio indicates flattening of the cord, which is commonly seen in degenerative cervical myelopathy, disc–osteophyte complexes, ossification of the posterior longitudinal ligament (OPLL), and chronic canal stenosis. The compression ratio correlates with neurologic deficit severity and functional outcomes, often complementing cord cross-sectional area (CSA) and canal measurements.
2) Instructions to Measure
Select a true axial T2-weighted MRI slice at:
The level of maximal cord compression, or
A standardized level (e.g., disc level) for serial comparisons.
Identify the outer margin of the spinal cord, defined by the interface between cord parenchyma and surrounding CSF.
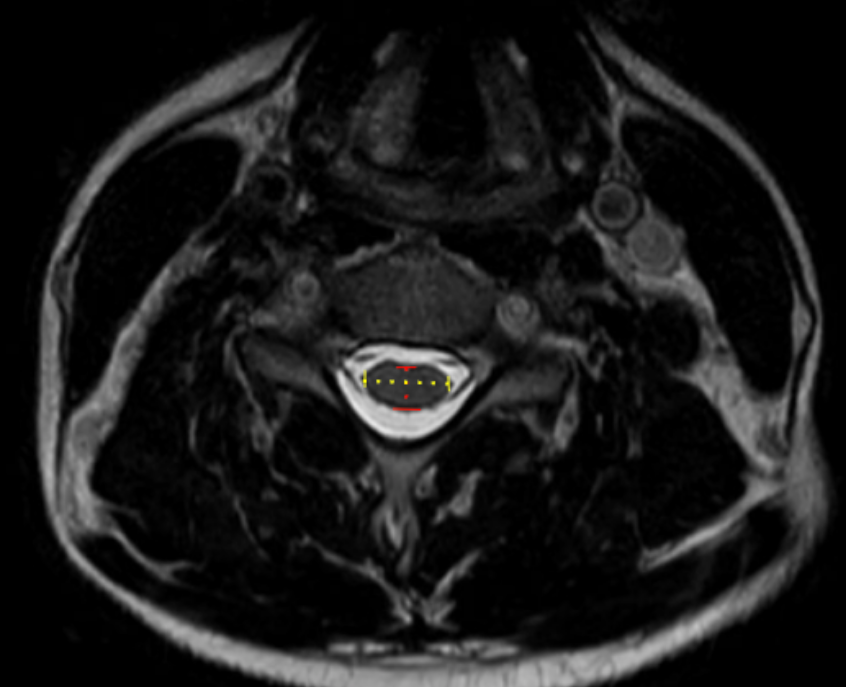
Measure the Anteroposterior (AP) cord diameter:
Draw a straight line from the anterior surface of the cord to the posterior surface of the cord.
Ensure the line is perpendicular to the transverse axis.
Measure the Transverse (left–right) cord diameter:
Draw a straight line across the widest horizontal dimension of the cord at the same level.
Calculate the Compression Ratio:
Compression Ratio = AP Cord Diameter/Transverse Cord Diameter
If multiple levels are evaluated, record the lowest ratio, as this represents the most severe compression.
3) Normal vs. Pathologic Ranges
Normal/minimal compression: ≥ 0.50
Mild compression: 0.4 - 0.49
Moderate compression: 0.3 - 0.39
Severe compression: < 0.3; high myelopathy risk
Key points:
Ratios < 0.40 are frequently associated with clinical myelopathy
Ratios < 0.30 correlate with poor neurologic recovery after decompression
4) Important References
Takao T, Morishita Y, Okada S, et al. Clinical relationship between cervical spinal canal stenosis and traumatic cervical spinal cord injury without major fracture or dislocation. Eur Spine J. 2013 Oct;22(10):2228-31. doi: 10.1007/s00586-013-2865-7. Epub 2013 Jun 23.
Kitagawa T, Fujiwara A, Kobayashi N, et al. Morphologic changes in the cervical neural foramen due to flexion and extension: in vivo imaging study. Spine (Phila Pa 1976). 2004 Dec 15;29(24):2821-5. doi: 10.1097/01.brs.0000147741.11273.1c.
Fehlings MG. Current Knowledge in Degenerative Cervical Myelopathy. Neurosurg Clin N Am. 2018 Jan;29(1):xiii-xiv. doi: 10.1016/j.nec.2017.09.021. Epub 2017 Oct 23.
Jannelli G, Nouri A, Molliqaj G, et al. Degenerative Cervical Myelopathy: Review of Surgical Outcome Predictors and Need for Multimodal Approach. World Neurosurg. 2020 Aug;140:541-547. doi: 10.1016/j.wneu.2020.04.233. Epub 2020 May 8.
5) Other info....
The compression ratio is independent of patient size, making it useful across populations
Particularly valuable for:
Comparing severity across patients
Tracking progression over time
Predicting postoperative neurologic recovery
Should be interpreted in conjunction with:
Cord cross-sectional area (CSA)
Canal cross-sectional area
Sagittal canal diameter
T2 cord signal change
A low compression ratio without T2 hyperintensity may still represent chronic cord deformation
Static MRI does not assess dynamic compression; consider flexion-extension radiographs if instability is suspected
Adapted from: https://www.mriclinicalcasemap.philips.com/global/case/75/i