
Image Type
Cord Cross-Sectional Area (CSA)
1) Description of Measurement
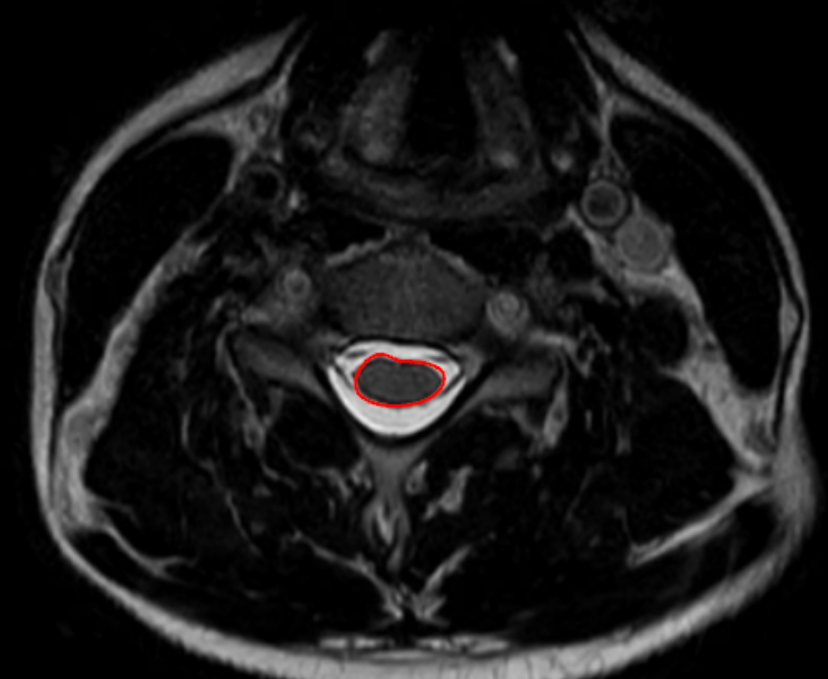
Cord cross-sectional area (CSA) quantifies the total area of the cervical spinal cord on axial MRI and is a direct morphologic marker of cord size, compression, and atrophy.
CSA is particularly valuable in the assessment of degenerative cervical myelopathy (DCM), traumatic injury, congenital stenosis, and chronic compressive lesions, as it reflects both acute deformation and chronic cord remodeling. Reduced CSA correlates strongly with neurologic deficit severity, disease chronicity, and functional outcomes, often more closely than canal measurements alone.
2) Instructions to Measure
Select a true axial T2-weighted MRI slice at the level of interest, preferably:
At the site of maximal compression, or
At a standardized level (e.g., mid-vertebral body or disc level for serial comparison)
Identify the outer boundary of the spinal cord, visualized as the interface between:
Cord parenchyma (intermediate signal), and
Surrounding cerebrospinal fluid (high T2 signal)
Using a freehand region-of-interest (ROI) tracing tool:
Carefully trace the outer margin of the spinal cord, excluding CSF, dura, and nerve roots.
Close the ROI to obtain an automated CSA calculation (mm²).
For comprehensive evaluation:
Repeat measurements at adjacent levels.
Record the smallest CSA, as this represents the point of maximal cord compromise.
3) Normal vs. Pathologic Ranges
Normal cervical cord: ≥ 70-80 mm2
Mild cord compression: 60-70 mm2
Moderate compression: 50-60 mm2; high risk for myelopathy
Severe compression: < 50 mm2; cord atrophy
Key points:
CSA < 60 mm² is frequently associated with clinical myelopathy
CSA < 50 mm² correlates with poorer neurologic recovery after decompression
4) Important References
Takao T, Morishita Y, Okada S, et al. Clinical relationship between cervical spinal canal stenosis and traumatic cervical spinal cord injury without major fracture or dislocation. Eur Spine J. 2013 Oct;22(10):2228-31. doi: 10.1007/s00586-013-2865-7. Epub 2013 Jun 23.
Kato F, Yukawa Y, Suda K, et al. Normal morphology, age-related changes and abnormal findings of the cervical spine. Part II: Magnetic resonance imaging of over 1,200 asymptomatic subjects. Eur Spine J. 2012 Aug;21(8):1499-507. doi: 10.1007/s00586-012-2176-4.
Fehlings MG. Current Knowledge in Degenerative Cervical Myelopathy. Neurosurg Clin N Am. 2018 Jan;29(1):xiii-xiv. doi: 10.1016/j.nec.2017.09.021. Epub 2017 Oct 23.
Jannelli G, Nouri A, Molliqaj G, et al. Degenerative Cervical Myelopathy: Review of Surgical Outcome Predictors and Need for Multimodal Approach. World Neurosurg. 2020 Aug;140:541-547. doi: 10.1016/j.wneu.2020.04.233. Epub 2020 May 8.
5) Other info…
Cord CSA is best measured on axial MRI, not sagittal views
Particularly useful for:
Monitoring disease progression
Predicting postoperative recovery
Differentiating acute compression from chronic cord atrophy
Should be interpreted alongside:
Canal cross-sectional area
Sagittal canal diameter
Pavlov–Torg ratio
T2 cord signal change
A reduced CSA without T2 hyperintensity may still represent chronic injury
Advanced techniques (DTI, MT imaging) can further characterize microstructural injury but CSA remains the most clinically practical quantitative metric
Adapted from: https://www.mriclinicalcasemap.philips.com/global/case/75/i