Image Type
Ullman’s Line
1) Description of Measurement
Sacral Slope (SS) is a fundamental spinopelvic parameter that quantifies the inclination of the sacral endplate relative to the horizontal plane. It reflects the anterior-posterior tilt of the sacrum and directly influences lumbar lordosis and overall sagittal spinal alignment.
A higher sacral slope indicates a more anteriorly inclined sacrum, correlating with greater lumbar lordosis and forward pelvic orientation. Conversely, a lower sacral slope corresponds to posterior pelvic tilt and flattening of lumbar curvature.
Sacral slope, along with pelvic tilt (PT) and pelvic incidence (PI), forms the triad of spinopelvic parameters critical to assessing sagittal balance, surgical planning, and postoperative alignment in both degenerative and deformity contexts.
2) Instructions to Measure
Obtain a standing lateral lumbosacral X-ray, ensuring visualization of the sacrum, pelvis, and lower lumbar spine.
Identify the superior endplate of the first sacral vertebra (S1).
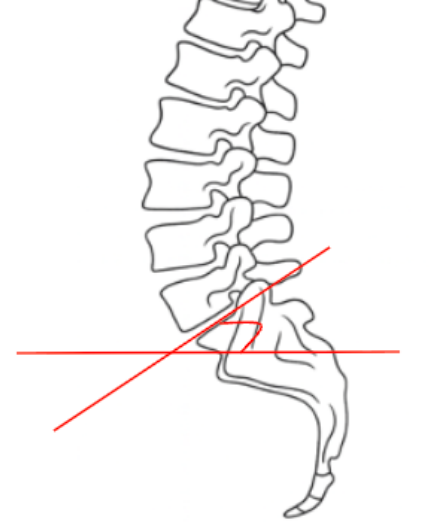
Draw a line along the superior endplate of S1 — this represents the sacral base line.
Draw a horizontal reference line (parallel to the bottom edge of the radiograph).
Measure the angle formed between the sacral base line and the horizontal line.
The angle opens anteriorly and is measured anterior to the sacrum.
Record the result in degrees (°) as the Sacral Slope (SS).
Ensure the X-ray is taken in a neutral, upright posture for accurate comparison across studies.
3) Normal vs. Pathologic Ranges
Normal range (SS): 30-50°; balanced sacropelvic alignment
Decreased/hypolordotic SS: < 30°; posterior pelvic tilt, flat-back posture, reduced lumbar lordosis
Increased/hyperlordotic SS: > 50°; anterior pelvic tilt, compensatory lordosis, potential spondylolisthesis
Key Points:
SS is directly proportional to lumbar lordosis—as SS increases, lumbar curvature deepens.
Changes in SS often represent pelvic compensation for sagittal imbalance.
Postoperative under-correction of SS can contribute to flat-back deformity or persistent positive sagittal balance.
4) Important References
Legaye J, Duval-Beaupère G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7(2):99–103.
Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005;87(2):260–267.
Le Huec JC, Aunoble S, Philippe L, Nicolas P. Pelvic parameters: origin and significance. Eur Spine J. 2011;20(Suppl 5):564–571.
Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis. Spine. 2005;30(3):346–353.
Barrey C, Roussouly P, Perrin G, Le Huec JC. Sagittal balance disorders in severe degenerative spine: can we identify the compensatory mechanisms? Eur Spine J. 2011;20(Suppl 5):626–633.
5) Other info....
Sacral Slope (SS) is the most dynamic spinopelvic parameter, varying with posture — unlike Pelvic Incidence (PI), which is fixed anatomically.
SS changes during sitting, standing, and bending as the pelvis tilts anteriorly or posteriorly to maintain sagittal balance.
In surgical planning, restoring an appropriate SS (and thus lumbar lordosis) is essential for achieving harmonious spinopelvic alignment.
SS should always be interpreted in conjunction with PT and PI for a complete assessment:
High SS → corresponds with high PI and large lumbar lordosis.
Low SS → correlates with flat-back posture and loss of physiologic curvature.
Restoration targets:
PI–LL mismatch ≤ 10° and SS appropriate to PI are ideal for postoperative balance.
In adult spinal deformity, SS serves as a real-time indicator of compensatory pelvic mechanics during stance.