Image Type
Pelvic Incidence-Slip Angle Relationship
1) Description of Measurement
The Pelvic Incidence–Slip Angle Relationship describes the geometric and biomechanical connection between pelvic morphology and lumbosacral kyphosis in spondylolisthesis.
It integrates two fundamental sagittal parameters:
Pelvic Incidence (PI): a fixed anatomical parameter reflecting the pelvis’s ability to accommodate spinal alignment.
Slip Angle (Lumbosacral Kyphosis Angle): a dynamic measurement quantifying the angular deformity between L5 and S1.
The relationship between these two parameters defines the severity of sagittal imbalance, risk of progression, and surgical correction goals in spondylolisthesis.
A high PI is commonly associated with greater lumbosacral kyphosis and increased slip angle, while low PI indicates a more vertical sacrum and reduced shear stress.
Understanding the PI–Slip Angle interplay is essential in classification (e.g., Labelle’s pelvic balance types) and surgical planning to restore sagittal harmony.
2) Instructions to Measure
Obtain a standing lateral lumbosacral X-ray including the pelvis, sacrum, and L5 vertebra.
Identify key anatomic landmarks:
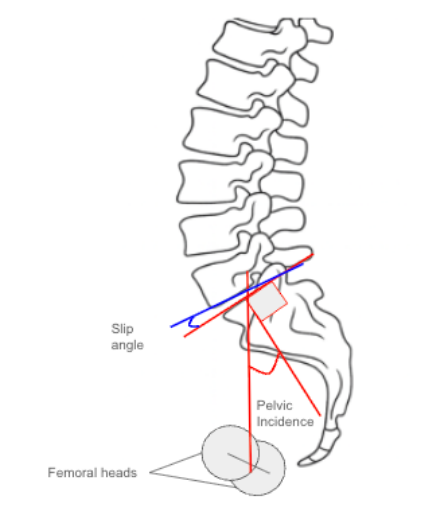
Center of the femoral heads (midpoint if both visible).
Center of the S1 superior endplate.
Inferior endplate of L5 and superior endplate of S1.
Measure Pelvic Incidence (PI):
Draw a line connecting the center of the femoral heads to the center of the S1 endplate.
Draw a line perpendicular to the S1 endplate.
The angle between these two lines is the Pelvic Incidence (PI).
Measure Slip Angle (Lumbosacral Kyphosis Angle):
Draw a line along the inferior endplate of L5.
Draw a line along the superior endplate of S1.
Measure the angle between these lines, which represents the Slip Angle.
Assess the Relationship:
Compare PI and Slip Angle values.
Larger PI–Slip Angle correlation indicates greater lumbosacral kyphosis and pelvic retroversion as compensatory mechanisms.
Record both measurements (in degrees) and document the alignment classification according to pelvic balance type (see below).
3) Normal vs. Pathologic Ranges
Normal PI: 40-60°; Low PI: < 40° (vertical sacrum); High PI: > 60° (oblique sacrum)
Normal Slip Angle: 0-10°; Lumbosacral kyphosis: > 20°; Severe Deformity: > 40°
PI-Slip Angle Relationship: Balanced if PI proportional to slip angle; imbalanced if slip angle disproportionately high relative to PI
Pelvic Balance Classification (Labelle et al.):
Balanced Pelvis: PI < 60°, Slip Angle < 30°
Unbalanced Pelvis: PI > 60°, Slip Angle > 30°
- Indicates higher risk of sagittal decompensation and poorer compensatory potential.
Key Insight:
The greater the difference between PI and Slip Angle, the more pronounced the sagittal malalignment and compensatory pelvic retroversion.
4) Important References
Labelle H, Mac-Thiong JM, Roussouly P, et al. Spino-pelvic alignment after surgical correction for developmental spondylolisthesis. Eur Spine J. 2011;20(Suppl 5):817–825.
Hresko MT, Labelle H, Roussouly P, Berthonnaud E. Classification of high-grade spondylolisthesis based on pelvic balance: the importance of sagittal alignment. Spine. 2007;32(20):2208–2213.
Mac-Thiong JM, Labelle H, Parent S, et al. Sagittal spinopelvic balance in lumbosacral spondylolisthesis: a comparison between high-grade and low-grade slips. Spine. 2008;33(5):487–492.
Boxall D, Bradford DS, Winter RB, Moe JH. Management of severe spondylolisthesis in children and adolescents. J Bone Joint Surg Am. 1979;61(4):479–495.
Dubousset J, Herring JA, Shufflebarger H. Spondylolisthesis in children and adolescents. Spine. 1999;24(24):2640–2648.
5) Other info....
The PI–Slip Angle Relationship forms the foundation of modern spondylolisthesis classification systems, correlating pelvic morphology with sagittal deformity.
High PI → increased shear stress at the lumbosacral junction, greater risk for high-grade slips.
Low PI → vertical sacrum, reduced shear, and less slip progression potential.
In high-grade spondylolisthesis, surgical goals include:
Reducing the slip angle to restore near-neutral lumbosacral alignment.
Preserving global sagittal balance relative to PI.
Ideal postoperative targets:
Slip Angle < 20°, PI–LL mismatch ≤ 10°, and restoration of pelvic balance.
The relationship also predicts compensatory mechanisms:
High PI → increased lumbar lordosis, pelvic retroversion, and knee flexion.
Low PI → limited compensation, often requiring anatomic reduction for balance restoration.
Advanced Imaging (EOS or CT) may improve precision for angular calculations and 3D modeling.