Image Type
Pelvic Tilt (PT)
1) Description of Measurement
Pelvic Tilt (PT) is a key spinopelvic parameter that measures the angular relationship between the pelvis and the vertical axis. It quantifies the degree of pelvic retroversion or anteversion, reflecting how the pelvis compensates for sagittal imbalance.
A higher pelvic tilt indicates posterior pelvic rotation (retroversion) — a compensatory mechanism often seen in patients with sagittal malalignment to maintain an upright posture. Conversely, a lower PT reflects anterior rotation (anteversion), typical of a balanced spine.
PT, in combination with Sacral Slope (SS) and Pelvic Incidence (PI), defines pelvic orientation and is critical for assessing sagittal alignment and planning corrective spine surgery.
2) Instructions to Measure
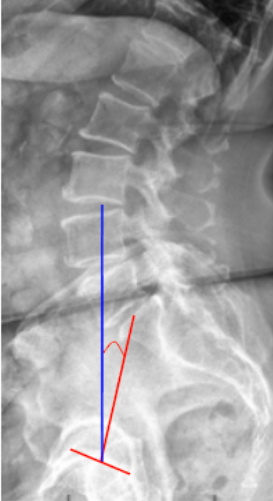
Obtain a standing lateral lumbosacral X-ray with visualization of the femoral heads and sacrum.
Identify two key anatomical landmarks:
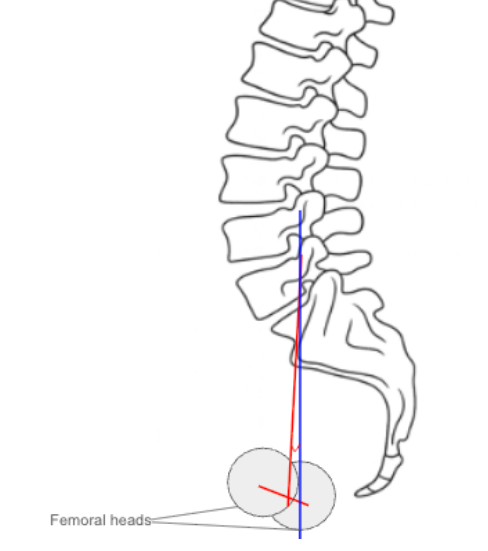
The center of the S1 endplate (midpoint of the superior sacral endplate).
The center of the femoral heads (use the midpoint if both are visible).
Draw a line connecting the center of the femoral heads to the center of the S1 endplate — this represents the pelvic axis.
Draw a vertical reference line perpendicular to the horizontal plane.
Measure the angle between the pelvic axis line and the vertical line — this is the Pelvic Tilt (PT).
The angle opens posteriorly, increasing with pelvic retroversion.
Record the angle in degrees (°).
3) Normal vs. Pathologic Ranges
Normal Range (PT): 10-20°; balanced pelvis; neutral alignment
Decreased/anteverted PT: < 10°; anterior pelvic rotation; increased sacral slope
Increased/retroverted PT: > 20-30°; posterior pelvic tilt; early compensation for sagittal imbalance
Markedly increased PT: > 30°; decompensated sagittal imbalance: energy-inefficient posture
Key Point:
Pelvic Tilt > 25° often indicates significant pelvic compensation secondary to loss of lumbar lordosis or positive sagittal vertical axis (SVA) shift.
4) Important References
Legaye J, Duval-Beaupère G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7(2):99–103.
Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005;87(2):260–267.
Le Huec JC, Aunoble S, Philippe L, Nicolas P. Pelvic parameters: origin and significance. Eur Spine J. 2011;20(Suppl 5):564–571.
Barrey C, Roussouly P, Perrin G, Le Huec JC. Sagittal balance disorders in severe degenerative spine: can we identify the compensatory mechanisms? Eur Spine J. 2011;20(Suppl 5):626–633.
Schwab F, Lafage V, Boyce R, Skalli W, Farcy JP. Gravity line analysis in adult volunteers: age-related correlation with spinal and pelvic parameters. Spine. 2006;31(25):E959–E967.
5) Other info....
PT is a dynamic parameter that changes with posture and compensatory mechanisms; it increases with posterior pelvic rotation when the spine loses lordosis.
It serves as a functional indicator of compensation, contrasting with Pelvic Incidence (PI), which is fixed anatomically.
High PT is seen in patients with sagittal imbalance, degenerative lumbar kyphosis, or after inadequate lumbar fusion correction.
Low PT may suggest a hyperlordotic or anteriorly shifted posture.
Target values for balanced sagittal alignment postoperatively often include:
PI–LL mismatch ≤ 10°,
PT < 25°,
SVA < 50 mm.
Restoration of appropriate PT contributes to energy-efficient posture and improved functional outcomes.
EOS or stitched long-cassette radiographs are preferred for precise and reproducible pelvic parameter measurement.