
Image Type
Lenke Classification
1) Description of Measurement
The Lenke Classification System is the contemporary standard for classifying adolescent idiopathic scoliosis (AIS). It defines scoliosis patterns in three dimensions by integrating: (1) Coronal curve type (1-6) to identify the major curve and structural characteristics of the minor curves, (2) Lumbar spine modifier (A, B, C) based on the relationship of the lumbar curve to the central sacral vertical line (CSVL), and (3) Thoracic sagittal modifier (-, N, +) based on its impact on the curvature from T5-T12.
This system distinguishes structural vs non-structural curves, enabling surgeons to determine which curves require inclusion in fusion constructs.
2) Instructions to Measure
Identify curve Type
Obtain four radiographs of the spine (standing long cassette coronal and sagittal, as well as right and left supine bending)
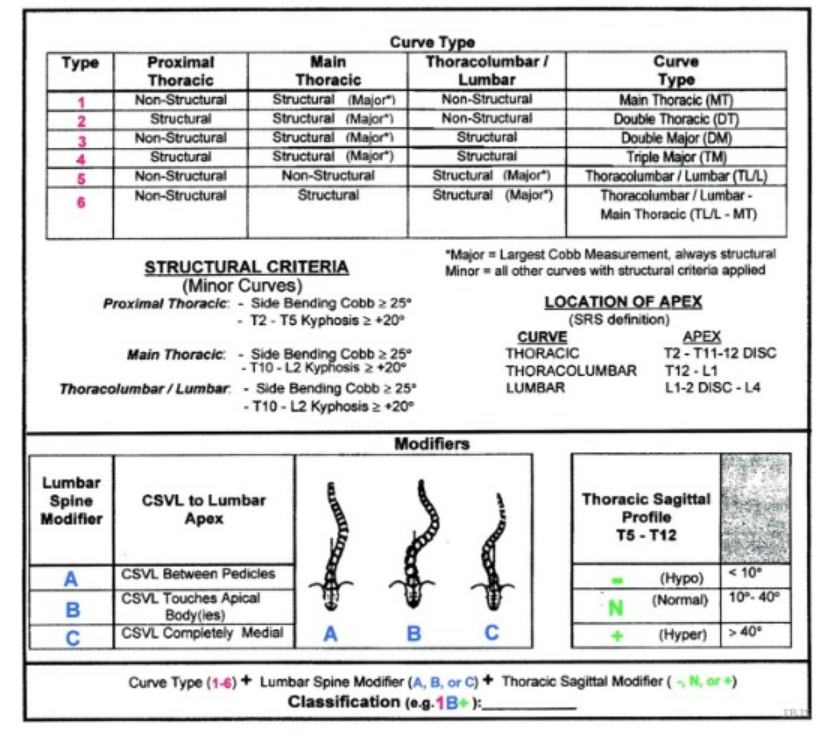
Structural Criteria:
Side bending Cobb angle ≥ 25°, or
Kyphosis
T2-T5 > 20° (proximal thoracic)
T10-L2 > 20° (thoracolumbar/lumbar)
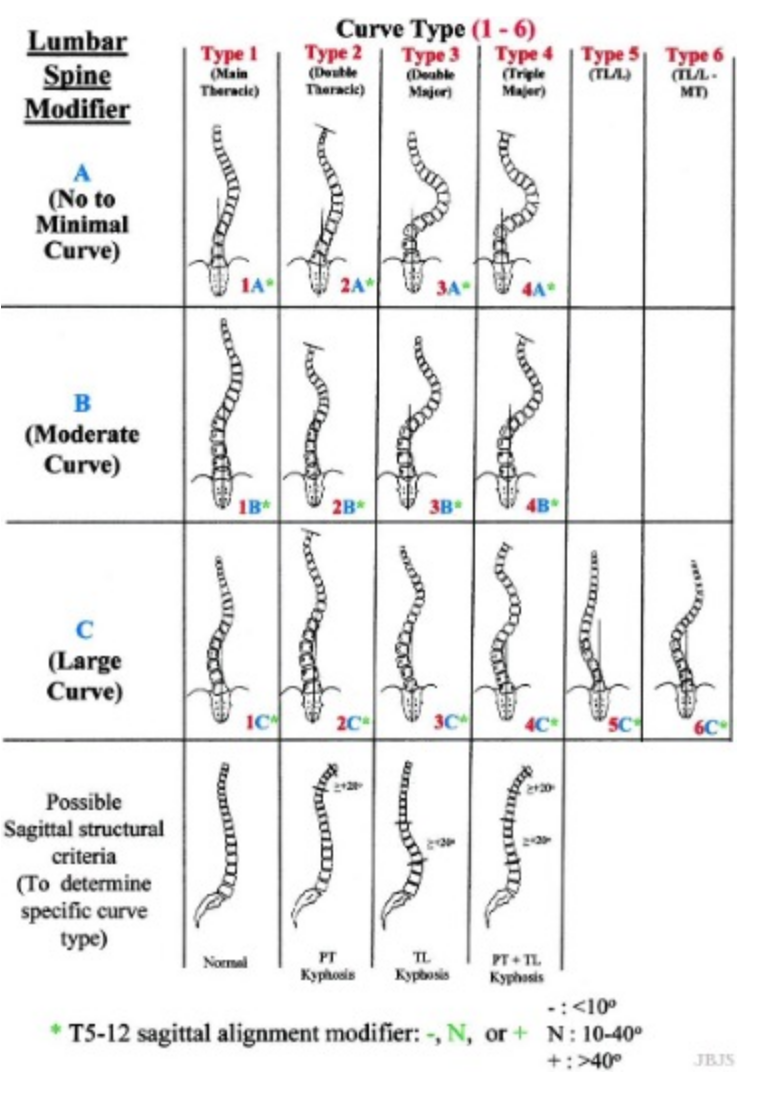
Curve Types:
Type 1: Main thoracic (structural MT)
Type 2: Double thoracic (structural PT and MT)
Type 3: Double major (structural MT and TL/L)
Type 4: Triple major (structural PT, MT*, TL/L*)
Type 5: Thoracolumbar/lumbar (structural TL/L)
Type 6: Thoracolumbar/lumbar-Main thoracic (structural MT and TL/L)
Structural proximal thoracic (PT) curves have Cobb angles of 25° on side-bending xrays and/or kyphosis between T2-T5 of ≥ 20°. Structural main thoracic (MT) curves have Cobb angles of 25° on side-bending xrays and/or kyphosis between T10-L2 of ≥ 20°. Structural thoracolumbar/lumbar (TL) curves have Cobb angles of 25° on side-bending xrays and/or kyphosis between T10-L2 of ≥ 20°. *Either the main thoracic or the thoracolumbar/lumbar curve can be the major curve.
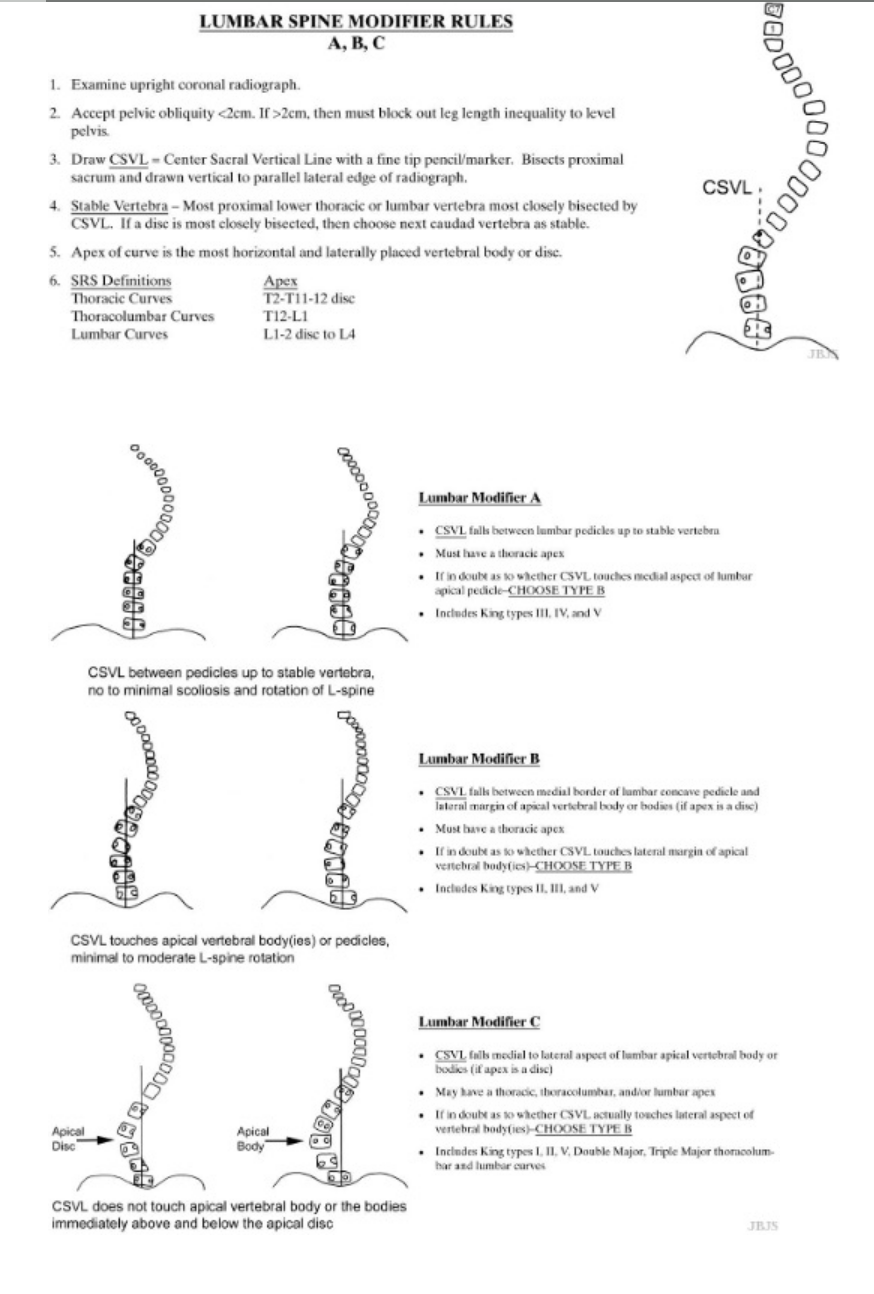
Assign Lumbar Modifier (A, B, C), Draw Central Sacral Vertical Line (CSVL)
A: CSVL passes between pedicles of stable/apical lumbar vertebra; thoracic apex; no/minimal scoliosis/rotation of lumbar spine (Types 1-4 only)
B: CSVL touches lumbar apical body; thoracic apex; minimal/moderate rotation of lumbar spine
C: CSVL medial to apical lumbar vertebra; main thoracic (Types 1-4), thoracolumbar, and/or lumbar apex (Types 5 and 6)
Assign Thoracic Sagittal Modifier, Measures T5-T12 kyphosis on lateral radiograph
(-): < 10° (hypokyphosis)
N: 10° - 40° (normal kyphosis)
(+): > 40° (hyperkyphosis)
3) Normal vs. Pathologic Ranges
Normal Side-bending Cobb: < 25°
Pathologic Side-bending Cobb: ≥ 25°; (structural deformity)
Normal T5-T12 Kyphosis: 10 - 40°
Hypo-/Hyperkyphosis: < 10° (-), >40 (+)
CSVL relative to Lumbar Apex (Normal): Between Pedicles (A)
CSVL relative to Lumbar Apex (Pathologic): Touching/medial to pedicles (B/C)
4) Important References
Lenke L, Betz R, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001; 83A: 1169–81.
Richards BS, Sucato DJ, Konigsberg DE, Ouellet JA. Comparison of reliability between the Lenke and King classification systems for adolescent idiopathic scoliosis using radiographs that were not premeasured. Spine (Phila Pa 1976). 2003 Jun 1;28(11):1148-56; discussion 1156-7. doi: 10.1097/01.BRS.0000067265.52473.C3.
Puno RM, An KC, Puno RL, Jacob A, Chung SS. Treatment recommendations for idiopathic scoliosis: an assessment of the Lenke classification. Spine (Phila Pa 1976). 2003 Sep 15;28(18):2102-14; discussion 2114-5. doi: 10.1097/01.BRS.0000088480.08179.35.
Lenke LG, Edwards CC 2nd, Bridwell KH. The Lenke classification of adolescent idiopathic scoliosis: how it organizes curve patterns as a template to perform selective fusions of the spine. Spine (Phila Pa 1976). 2003 Oct 15;28(20):S199-207. doi: 10.1097/01.BRS.0000092216.16155.33.
5) Other info....
The Lenke system determines fusion strategy:
Structural curves must be fused.
Non-structural curves may be spared to preserve motion.
It improved outcomes over King–Moe by:
Including sagittal alignment
Improving inter-observer reliability
Reducing postoperative coronal decompensation
Figures adapted from: Lenke LG, Betz RR, Harms J, Bridwell KH, Clements DH, Lowe TG, Blanke K. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am. 2001 Aug;83(8):1169-81.