
Image Type
King-Moe Classification
1) Description of Measurement
The King–Moe Classification is a historic coronal-plane classification system for adolescent idiopathic scoliosis (AIS) based on the relationship and dominance of thoracic and lumbar curves on standing AP radiographs. It was developed during the Harrington rod era of spinal deformity correction to guide selection of fusion levels by identifying the major curve pattern. The flexibility index (FI) was introduced with this system. This index assesses the percent of flexibility of the lumbar and thoracic curves on maximum lateral bending. The flexibility index is equal to the difference of the percent correction of the lumbar curve and percent correction of the thoracic curve.
The system describes five coronal curve types (Types I–V), focusing exclusively on coronal alignment (based on the central sacral vertical line) without considering sagittal profile or three-dimensional deformity.
2) Instructions to Measure
Obtain a standing erect AP radiograph of the entire spine.
Identify all coronal curves and measure the Cobb angle of:
The main thoracic curve
The lumbar or thoracolumbar curve
Determine which curve is the dominant (larger) curve.
Assess the location of the apices and whether the lumbar curve crosses the central sacral vertical line (CSVL).
Assign the curve pattern based on the shape of the curve, presence/absence of multiple curves, and extent of lumbar compensation
3) Normal vs. Pathologic Ranges
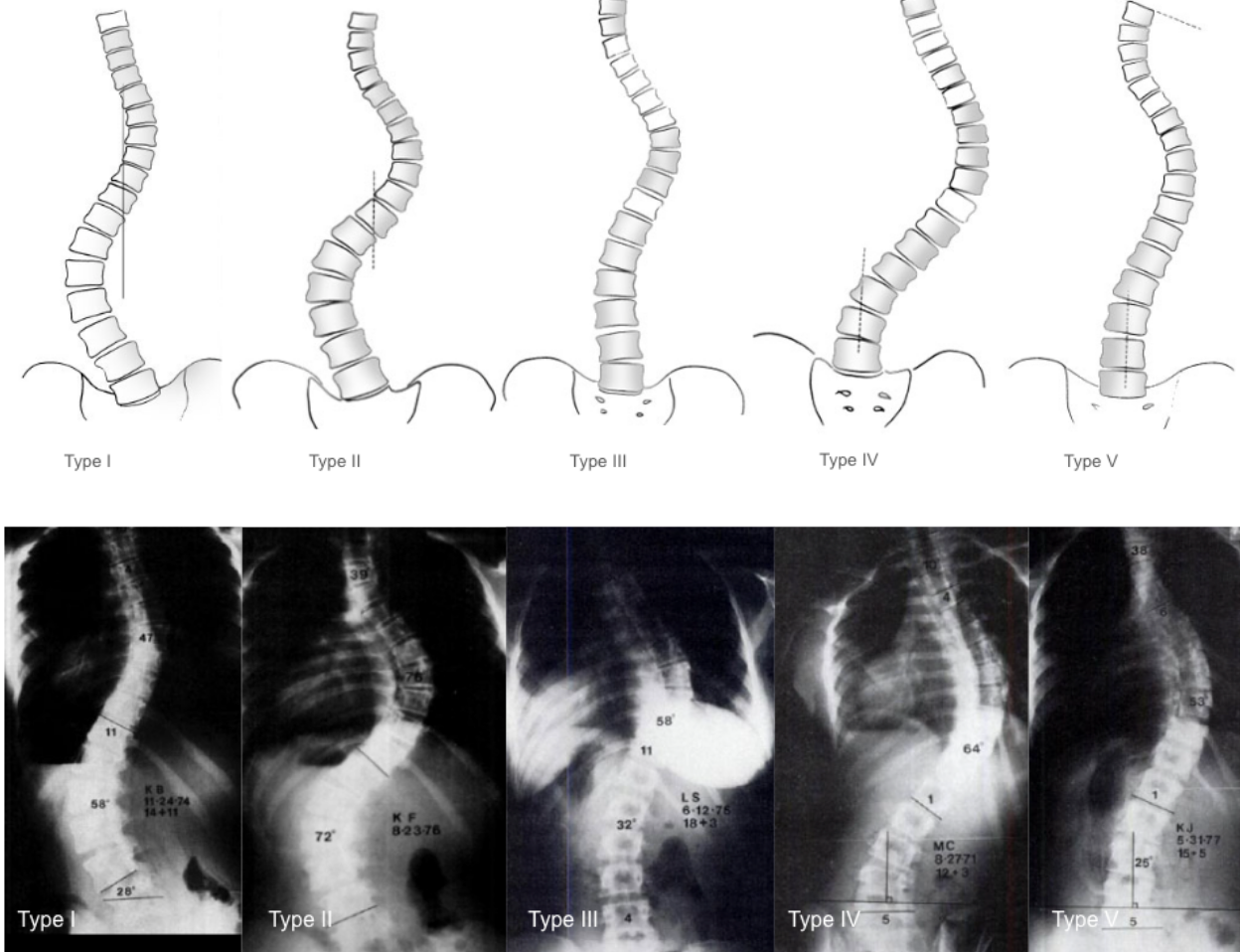
Type I: S-shaped (double curve) with both lumbar and thoracic curves crossing midline; lumbar curve generally larger and stiffer than thoracic curve; FI is generally negative (thoracic curve ≥ lumbar curve standing and more flexible with side-bending)
Type II: S-shaped (double curve) with both lumbar and thoracic curves crossing midline; thoracic curve generally larger and stiffer than lumbar curve; FI generally positive
Type III: Prominent thoracic curve with minimal lumbar compensation (does not cross midline); thoracic ‘overhang’
Type IV: Long thoracic curve where L5 is positioned over sacrum but L4 tilts into thoracic curve
Type V: Double thoracic curve with T1 tilting into apex of upper curve; upper curve appears structural on side-bending
4) Important References
King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am. 1983 Dec;65(9):1302-13.
Smith JS, Shaffrey CI, Kuntz C 4th, Mummaneni PV. Classification systems for adolescent and adult scoliosis. Neurosurgery. 2008 Sep;63(3 Suppl):16-24. doi: 10.1227/01.NEU.0000320447.61835.EA.
Ritzman TF, Floccari LV. The Sagittal Plane in Spinal Fusion for Adolescent Idiopathic Scoliosis. J Am Acad Orthop Surg. 2022 Jul 15;30(14):e957-e967. doi: 10.5435/JAAOS-D-21-01060.
5) Other info....
Historical Role
Designed specifically to guide Harrington rod fusion levels.
Emphasized avoidance of postoperative coronal decompensation.
Key Limitations
Poor inter-observer reliability — different surgeons frequently assigned different curve types.
No sagittal plane assessment — does not account for thoracic kyphosis or lumbar lordosis.
No evaluation of curve flexibility.
Inadequate for modern segmental instrumentation strategies.
Modern Relevance
The King–Moe system has been largely replaced by the Lenke Classification, which incorporates:
Coronal pattern
Sagittal alignment
Curve flexibility
Adapted from: Moore DW. King Classification of AIS. 5 Oct 2016. (Accessed 29 Dec 2025). https://www.orthobullets.com/spine/2075/king-classification-of-ais