
Image Type
Side-bending Films (Coronal flexibility)
1) Description of Measurement
Side-bending films quantify coronal plane flexibility of scoliotic curves by measuring the residual Cobb angle during maximal right and left lateral bending. This measurement is used to determine whether a curve is structural or compensatory, to assess curve stiffness, and to guide operative planning, including the selection of fusion levels.
Coronal flexibility reflects the ability of a spinal curve to correct with active bending and correlates with disc, facet, and ligamentous elasticity.
2) Instructions to Measure
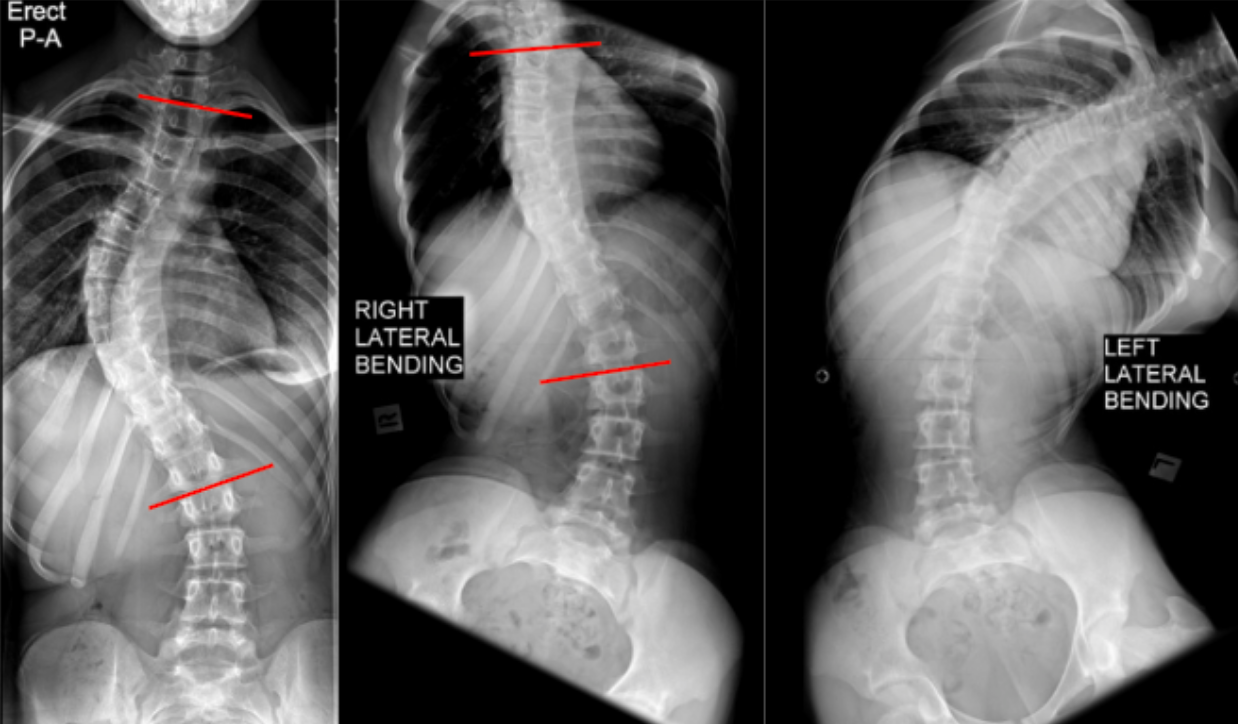
Obtain three full-length standing radiographs:
Erect AP
Maximal right lateral bending
Maximal left lateral bending
On the erect AP film, identify the major curve and measure the baseline Cobb angle using the standard end-vertebra method.
On the corresponding side-bending film (right or left, depending on curve convexity):
Identify the same superior and inferior end vertebrae used for the erect Cobb angle.
Measure the residual Cobb angle while the patient is maximally bent.
Calculate Coronal Flexibility (%):
Flexibility (%) = Erect Cobb - Bending CobbErect Cobb100
Record the lowest residual Cobb angle obtained during bending, as this represents maximal achievable correction.
3) Normal vs. Pathologic Ranges
High flexibility curve: > 50%
Moderately flexible: 30 - 50%
Rigid curve: < 30%
Structural, stiff deformity: Minimal/no change
Key points:
Curves with < 30% flexibility are typically considered structural
Highly flexible curves may not require inclusion in fusion constructs
4) Important References
Ohrt-Nissen S, Shigematsu H, Cheung JPY, et al. Predictability of Coronal Curve Flexibility in Postoperative Curve Correction in Adolescent Idiopathic Scoliosis: The Effect of the Sagittal Profile. Global Spine J. 2020 May;10(3):303-311. doi: 10.1177/2192568219877862.
Lenke LG, Edwards CC 2nd, Bridwell KH. The Lenke classification of adolescent idiopathic scoliosis: how it organizes curve patterns as a template to perform selective fusions of the spine. Spine (Phila Pa 1976). 2003 Oct 15;28(20):S199-207. doi: 10.1097/01.BRS.0000092216.16155.33.
King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am. 1983 Dec;65(9):1302-13.
Luk KD, Cheung KM, Lu DS, Leong JC. Assessment of scoliosis correction in relation to flexibility using the fulcrum bending correction index. Spine (Phila Pa 1976). 1998 Nov 1;23(21):2303-7. doi: 10.1097/00007632-199811010-00011.
5) Other info....
Side-bending films are critical for:
Distinguishing structural vs non-structural curves
Determining lowest instrumented vertebra (LIV)
Predicting postoperative coronal balance
Should be interpreted in conjunction with:
Standing AP Cobb angles
Sagittal profile
Clinical flexibility and rotation
In patients unable to actively bend, supine traction or push-prone films may be used as alternatives
Residual Cobb angle on bending is often more predictive of surgical correction potential than the baseline erect Cobb angle alone
Adapted from: Gaillard F, Scoliosis. Case study, Radiopaedia.org (Accessed on 28 Dec 2025) https://doi.org/10.53347/rID-49513