Image Type
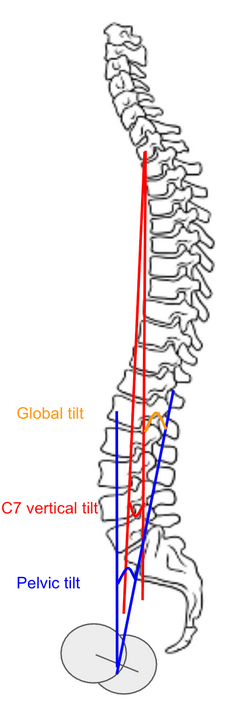
Global Tilt (C7 vertical tilt + pelvic tilt)
1) Description of Measurement
Global Tilt (C7 vertical tilt + pelvic tilt) is a comprehensive radiographic parameter that quantifies overall sagittal spinal alignment by combining spinal inclination (C7 vertical tilt) and pelvic retroversion (Pelvic Tilt).
It reflects the angular relationship between the upper spine and pelvis in maintaining upright posture, accounting for both thoracic inclination and pelvic compensation.
Mathematically:
Global Tilt = C7 Vertical Tilt + Pelvic Tilt
Global Tilt correlates strongly with sagittal balance, spinal deformity severity, and functional outcomes. It is particularly useful in adult spinal deformity (ASD) assessment as a posture-independent parameter that integrates global trunk alignment and pelvic compensation mechanisms.
2) Instructions to Measure
Obtain a standing lateral full-length spine X-ray, ensuring visualization from the cervical spine through the femoral heads.
Identify three key landmarks:
Center of C7 vertebral body (midpoint between anterior and posterior cortices).
Center of S1 endplate (midpoint of the superior sacral endplate).
Center of the femoral heads (use midpoint if both are visible).
Measure C7 Vertical Tilt (C7VT):
Draw a line from the center of C7 to the center of the femoral heads.
Measure the angle between this line and the vertical (gravity) reference line.
Measure Pelvic Tilt (PT):
Draw a line from the center of the femoral heads to the center of the S1 endplate.
Measure the angle between this line and the vertical reference line.
Calculate Global Tilt = C7VT + PT.
A larger Global Tilt reflects increased anterior spinal inclination and compensatory pelvic retroversion, indicating positive sagittal malalignment.
3) Normal vs. Pathologic Ranges
Normal sagittal alignment: < 35°; balanced global posture with minimal compensatory pelvic tilt
Mild imbalance: 35-45°; early sagittal malalignment; mild pelvic retroversion compensation
Moderate imbalance: 45-55°; significant trunk inclination and pelvic compensation
Severe imbalance: > 55°; global sagittal decompensation; high energy expenditure posture
Key Point:
Global Tilt > 45° is associated with reduced health-related quality of life and greater disability, often warranting sagittal realignment surgery in adult deformity.
4) Important References
Schwab F, Lafage V, Boyce R, Skalli W, Farcy JP. Gravity line analysis in adult volunteers: age-related correlation with spinal parameters, pelvic parameters, and foot position. Spine. 2006;31(25):E959–E967.
Protopsaltis TS, Lafage V, Vira S, et al. T1 pelvic angle (TPA): a novel radiographic measure of global sagittal deformity that accounts for both spinal inclination and pelvic retroversion. Spine. 2014;39(9):782–788.
Lafage R, Schwab F, Challier V, et al. Defining spino-pelvic alignment thresholds correlated with quality of life in adult spinal deformity. Spine. 2016;41(1):62–69.
Le Huec JC, Thompson W, Mohsinaly Y, Barrey C, Faundez A. Sagittal balance of the spine. Eur Spine J. 2019;28(9):1889–1905.
Obeid I, Boissiere L, Yilgor C, et al. Global tilt: a single parameter incorporating spinal and pelvic sagittal parameters and least affected by patient positioning. Eur Spine J. 2016 Nov;25(11):3644-3649.
5) Other info....
Global Tilt provides a posture-independent assessment of global sagittal alignment by combining spinal tilt (C7 vertical inclination) with pelvic compensation (pelvic tilt).
It offers a simpler alternative to the T1 Pelvic Angle (T1PA) when the upper thoracic vertebrae are obscured.
The angle captures both spinal inclination and pelvic retroversion, two main compensatory mechanisms for maintaining upright posture and horizontal gaze.
It is less affected by knee flexion or shoulder position than SVA, offering greater reproducibility.
Clinical correlations:
Global Tilt > 45° → increased disability, reduced energy efficiency.
Restoring Global Tilt < 40° postoperatively aligns with improved quality of life and reduced fatigue.
The measurement is particularly valuable in evaluating adult spinal deformity, flat-back syndrome, and post-fusion sagittal imbalance.
Use low-dose EOS imaging or stitched digital long-cassette X-rays for optimal accuracy.