Image Type
T4 Pelvic Angle (T4PA)
1) Description of Measurement
The T4 Pelvic Angle (T4PA) is a sagittal alignment parameter that evaluates global spinal balance, integrating both thoracic inclination and pelvic retroversion into a single angular measurement.
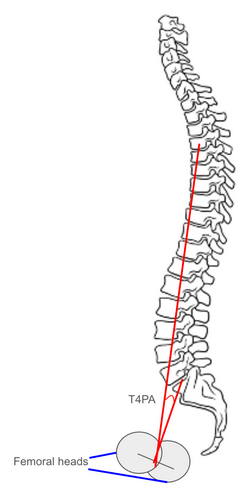
It is defined as the angle formed between two lines:
one drawn from the center of the T4 vertebral body to the center of the femoral heads, and
another from the center of the S1 endplate to the center of the femoral heads.
Unlike the Sagittal Vertical Axis (SVA), which is posture-dependent, T4PA provides a positional-independent metric that accounts for both upper spinal inclination and compensatory pelvic rotation.
T4PA reflects the thoracic contribution to sagittal alignment and is particularly valuable when assessing thoracic deformity correction, post-fusion compensation, and overall sagittal harmony.
2) Instructions to Measure
Obtain a standing lateral full-length spine X-ray, ensuring visualization from the cervical spine through the femoral heads. The patient should be upright, knees extended, and arms supported forward at shoulder height.
Identify the following anatomical landmarks:
Center of the T4 vertebral body (midpoint between anterior and posterior cortices).
Center of the S1 endplate (midpoint of the superior sacral endplate).
Center of the femoral heads (if both visible, use the midpoint of a line connecting the two).
Draw:
Line 1: from the center of T4 to the center of the femoral heads.
Line 2: from the center of S1 to the center of the femoral heads.
Measure the angle formed between Line 1 and Line 2 — this is the T4 Pelvic Angle (T4PA).
A larger T4PA indicates increased anterior spinal inclination and/or pelvic retroversion, signifying positive sagittal imbalance.
Report the T4PA in degrees (°), noting that it complements SVA and Pelvic Tilt in quantifying overall sagittal alignment.
3) Normal vs. Pathologic Ranges
Normal T4PA: <10°; balanced sagittal alignment; minimal thoracic inclination or pelvic retroversion
Mild imbalance: 10-20°; early compensation from thoracic or pelvic segments
Moderate imbalance: 20-30°; increased anterior trunk inclination; compensatory mechanisms active
Severe imbalance: > 30°; global sagittal decompensation; strong indication for surgical correction
Key Point:
T4PA > 20° is associated with increased disability, reduced energy efficiency, and postoperative dissatisfaction in adult spinal deformity (ASD) populations.
4) Important References
Protopsaltis TS, Lafage V, Vira S, et al. T1 pelvic angle (TPA): a novel radiographic measure of global sagittal deformity accounts for both spinal inclination and pelvic retroversion. Spine. 2014;39(9):782–788.
Lafage R, Schwab F, Challier V, et al. Defining spino-pelvic alignment thresholds correlated with quality of life in adult spinal deformity: standing alignment. Spine. 2016;41(1):62–69.
Yilgor C, Sogunmez N, Boissiere L, et al. Global alignment and proportion (GAP) score: predicting mechanical complications and HRQOL after adult spinal deformity surgery. Eur Spine J. 2017;26(8):2329–2338.
Smith JS, Shaffrey CI, Ames CP, et al. Assessment of global sagittal alignment in adult spinal deformity: integrating regional and pelvic parameters. Spine Deform. 2015;3(3):169–179.
Diebo BG, Oren JH, Lafage V, et al. Global spinal alignment in the setting of thoracic and lumbar deformity: importance of head position and pelvic compensation. Spine. 2016;41(19):1591–1598.
5) Other info....
T4PA is a variation of the T1 Pelvic Angle, shifting the upper reference point caudally to reduce measurement variability due to shoulder position and thoracic inlet obstruction.
It serves as a practical surrogate when T1 is not clearly visible on lateral radiographs, while maintaining correlation with global sagittal alignment parameters (R² ≈ 0.9 with T1PA).
T4PA combines thoracic inclination (spinal alignment) with pelvic tilt (compensation), offering a more complete picture of sagittal posture than SVA alone.
Target alignment goals in adult deformity correction:
T4PA ≤ 20°,
PI–LL mismatch ≤ 10°,
SVA ≤ 40 mm.
These thresholds collectively define postoperative sagittal balance.
Larger T4PA values correlate with increased fatigue, forward stooping, and functional disability, and reduction of T4PA postoperatively reflects improved posture restoration.
Use EOS low-dose imaging or stitched digital long-cassette X-rays for maximal accuracy and minimal projection error.
Always interpret T4PA in conjunction with thoracic kyphosis, lumbar lordosis, and pelvic parameters to fully characterize spinopelvic balance.