
Image Type
Cincinnati/PUMC Classification Systems
1) Description of Measurement
The Cincinnati / PUMC Classification System is an operative classification for adolescent idiopathic scoliosis (AIS) designed to improve reliability and to directly guide surgical fusion strategy. Unlike earlier systems, it incorporates not only coronal curve morphology, but also curve magnitude, flexibility, apical rotation, stable vertebra, and thoracolumbar sagittal alignment.
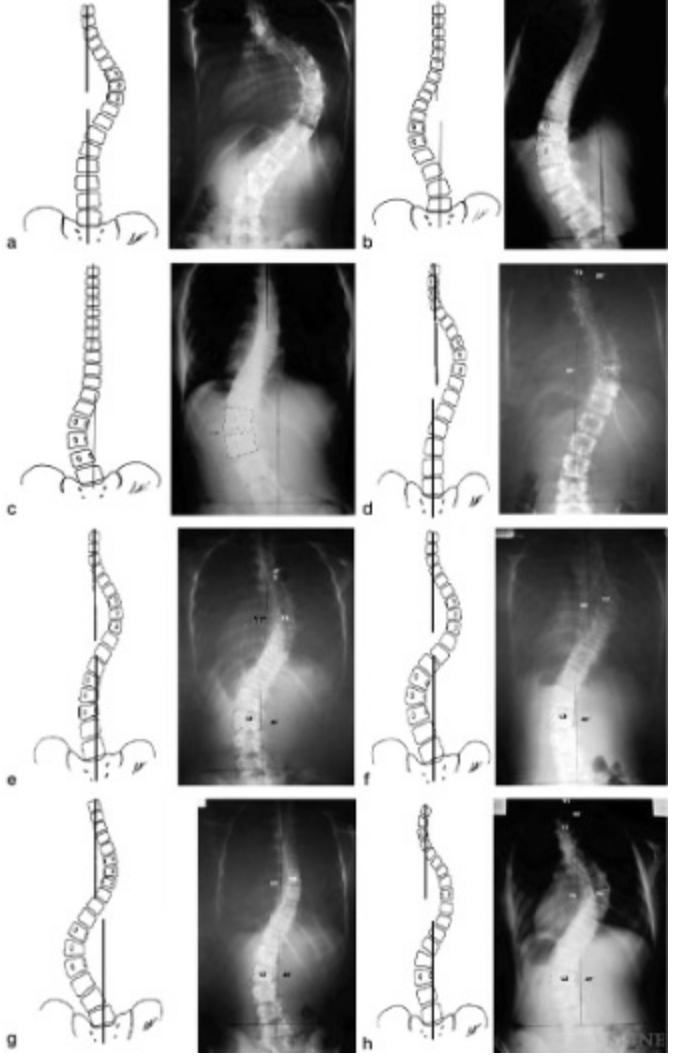
Curves are divided into three major types based on number of apices:
Type I: Single curve
Type II: Double curves
Type III: Triple curves
These are subdivided into Ia, Ib, Ic, IIa, IIb, IIc, IId, IIIa, and IIIb, each with distinct morphologic patterns and fusion guidelines.
2) Instructions to Measure
For each patient obtain standing AP, lateral, and supine side-bending radiographs.
Record the following parameters:
Cobb Angle
Measure Cobb angle for each curve.
A curve is defined when Cobb angle >10°.
Flexibility (%):
Flexibility = Standing Cobb - Convex Bending CobbStanding Cobb100
Apical Vertebral Rotation
Grade rotation using the Nash-Moe method (Grade 0-4)
Stable Vertebra
Identify the most distal vertebra bisected by the Central Sacral Vertical Line (CSVL)
Thoracolumbar Kyphosis
Measure sagittal Cobb angle between T12-L1
Kyphosis is defined as angle > 0°
3) Normal vs. Pathologic Ranges
Normal Cobb Angle: < 10°
Pathologic Cobb Angle: ≥ 10° (defines scoliosis)
Normal Curve dominance: Difference < 10° = equivalent
Pathologic Curve dominance: Difference ≥ 10° = larger vs minor curve
Normal Flexibility: > 70%
Pathologic Flexibility: < 50% (rigid)
Normal Apical rotation (Nash-Moe): Grade 0-I
Pathologic Apical rotation (Nash-Moe): ≥ Grade II (significant)
Normal thoracolumbar kyphosis: 0°
Pathologicc thoracolumbar kyphosis: > 0° indicates kyphotic TL junction
4) Important References
Qiu G, Zhang J, Wang Y, et al. A new operative classification of idiopathic scoliosis: a peking union medical college method. Spine (Phila Pa 1976). 2005 Jun 15;30(12):1419-26. doi: 10.1097/01.brs.0000166531.52232.0c.
Nash CL Jr, Moe JH. A study of vertebral rotation. J Bone Joint Surg Am. 1969 Mar;51(2):223-9.
Qiu G, Zhang J, Wang Y, et al. A new operative classification of idiopathic scoliosis: a peking union medical college method. Spine (Phila Pa 1976). 2005 Jun 15;30(12):1419-26. doi: 10.1097/01.brs.0000166531.52232.0c.
5) Other info....(Curve Types and Surgical Logic)
Type Ia: Single thoracic (Apex T2-T11/12)
Type Ib: Single thoracolumbar (TL/L) (Apex T12-L1)
Type Ic: Single lumbar (Apex L1-L4/5)
Type IIa: Double thoracic (Two thoracic apices)
Type IIb: Thoracic + TL/L (thoracic ≥ 10° larger)
Selective thoracic fusion if lumbar Cobb ≤ 45°, flexibility ≥70%, rotation ≤ Grade I
Type IIc: Thoracic + TL/L (difference <10°)
Fusion based on relative flexibility
Type IId: Thoracic + TL/L (lumbar ≥10° larger)
Selective lumbar if thoracic flexible
Type IIIa: Triple curves – distal flexible
Fuse proximal two curves
Type IIIb: Triple curves – distal rigid
Fuse all three curves
Adapted from: Qiu G, Zhang J, Wang Y, et al. A new operative classification of idiopathic scoliosis: a peking union medical college method. Spine (Phila Pa 1976). 2005 Jun 15;30(12):1419-26. doi: 10.1097/01.brs.0000166531.52232.0c.