Image Type
L1 Pelvic Angle (L1PA)
1) Description of Measurement
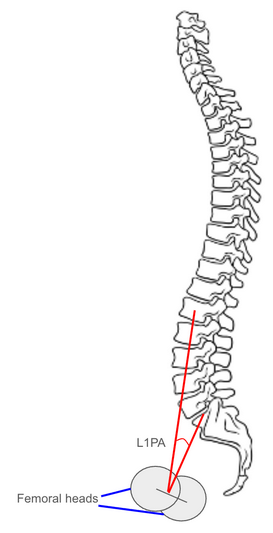
The L1 Pelvic Angle (L1PA) is a radiographic parameter used to evaluate global sagittal alignment by incorporating both spinal inclination and pelvic retroversion.
It is defined as the angle formed between two lines: one connecting the center of the L1 vertebral body to the center of the femoral heads, and the other connecting the center of the S1 endplate to the center of the femoral heads.
The L1PA is a modification of the T1 Pelvic Angle (T1PA) and provides a more lumbar-focused representation of sagittal deformity, particularly useful when upper thoracic landmarks (like T1) are obscured or when analyzing lumbar-pelvic compensation.
It correlates strongly with global sagittal imbalance, lumbar lordosis deficiency, and pelvic tilt, serving as a posture-independent measure of sagittal deformity severity.
2) Instructions to Measure
Obtain a standing lateral full-length spine X-ray, ensuring visualization of the spine from the occiput through the femoral heads.
Identify the following landmarks:
Center of the L1 vertebral body (midpoint between anterior and posterior cortices).
Center of the S1 endplate (midpoint of the superior sacral endplate).
Center of the femoral heads (midpoint between the centers if both are visible).
Draw the following lines:
Line 1: from the center of L1 to the center of the femoral heads.
Line 2: from the center of S1 endplate to the center of the femoral heads.
Measure the angle formed between Line 1 and Line 2 — this is the L1 Pelvic Angle (L1PA).
Record the angle in degrees (°).
A larger angle reflects greater anterior spinal inclination and pelvic retroversion, indicating positive sagittal malalignment.
A smaller angle indicates normal alignment or balanced posture.
For consistency, ensure neutral stance (knees extended, gaze horizontal) and the same reference points in follow-up imaging.
3) Normal vs. Pathologic Ranges
Normal sagittal alignment: < 10°; balanced posture; physiologic lumbar-pelvic alignment
Mild sagittal imbalance: 10-20°; early compensation by pelvic retroversion
Moderate sagittal imbalance: 20-30°; combined anterior spinal lean and pelvic tilt; functional fatigue common
Severe sagittal imbalance: > 30°; global malalignment with marked compensatory mechanisms; surgical correction typically indicated
Key Point:
L1PA correlates with both T1PA and Sagittal Vertical Axis (SVA) but is less affected by variations in thoracic curvature or shoulder positioning, offering a stable alternative when upper thoracic landmarks are not visible.
4) Important References
Protopsaltis TS, Lafage V, Vira S, et al. T1 pelvic angle (TPA): a novel radiographic measure of global sagittal deformity accounts for both spinal inclination and pelvic retroversion. Spine. 2014;39(9):782–788.
Lafage R, Schwab F, Challier V, et al. Defining spino-pelvic alignment thresholds correlated with quality of life in adult spinal deformity: standing alignment. Spine. 2016;41(1):62–69.
Diebo BG, Oren JH, Lafage R, et al. Global spinal alignment and proportion score: integrating alignment targets into surgical planning. Spine J. 2017;17(2):193–199.
Le Huec JC, Faundez A, Dominguez D, Hoffmeyer P, Aunoble S. Equilibrium of the human body and the gravity line: the basics. Eur Spine J. 2011;20(Suppl 5):558–563.
Smith JS, Klineberg E, Schwab F, et al. The contribution of the L1 pelvic angle to sagittal balance analysis in adult spinal deformity. Spine Deform. 2020;8(3):463–472.
5) Other info....
The L1 Pelvic Angle reflects lumbar and lower thoracic contribution to overall sagittal balance, particularly useful in patients with thoracic fusions or limited upper thoracic visualization.
It is less sensitive to patient posture or knee flexion compared to the SVA, making it a more stable and reproducible measure of global alignment.
L1PA integrates the effects of spinal inclination and pelvic retroversion, two compensatory mechanisms that influence energy-efficient posture.
Strong correlations exist between L1PA, T1PA, and health-related quality-of-life metrics (ODI, SRS-22).
In adult spinal deformity surgery, alignment goals often target L1PA < 20° postoperatively to restore efficient standing posture.
When both T1 and L1 are visible, comparing T1PA and L1PA can reveal whether deformity is primarily thoracic-driven or lumbar-pelvic in origin.
EOS low-dose imaging provides superior measurement accuracy by minimizing projectional error and allowing 3D angle reconstruction.