
Spinal Deformity Classifications
King-Moe Classification
Adapted from: Moore DW. King Classification of AIS. 5 Oct 2016. (Accessed 29 Dec 2025). https://www.orthobullets.com/spine/2075/king-classification-of-ais
1) Description of Measurement
The King–Moe Classification is a historic coronal-plane classification system for adolescent idiopathic scoliosis (AIS) based on the relationship and dominance of thoracic and lumbar curves on standing AP radiographs. It was developed during the Harrington rod era of spinal deformity correction to guide selection of fusion levels by identifying the major curve pattern. The flexibility index (FI) was introduced with this system. This index assesses the percent of flexibility of the lumbar and thoracic curves on maximum lateral bending. The flexibility index is equal to the difference of the percent correction of the lumbar curve and percent correction of the thoracic curve.
The system describes five coronal curve types (Types I–V), focusing exclusively on coronal alignment (based on the central sacral vertical line) without considering sagittal profile or three-dimensional deformity.
2) Instructions to Measure
Obtain a standing erect AP radiograph of the entire spine.
Identify all coronal curves and measure the Cobb angle of:
The main thoracic curve
The lumbar or thoracolumbar curve
Determine which curve is the dominant (larger) curve.
Assess the location of the apices and whether the lumbar curve crosses the central sacral vertical line (CSVL).
Assign the curve pattern based on the shape of the curve, presence/absence of multiple curves, and extent of lumbar compensation
3) Normal vs. Pathologic Ranges
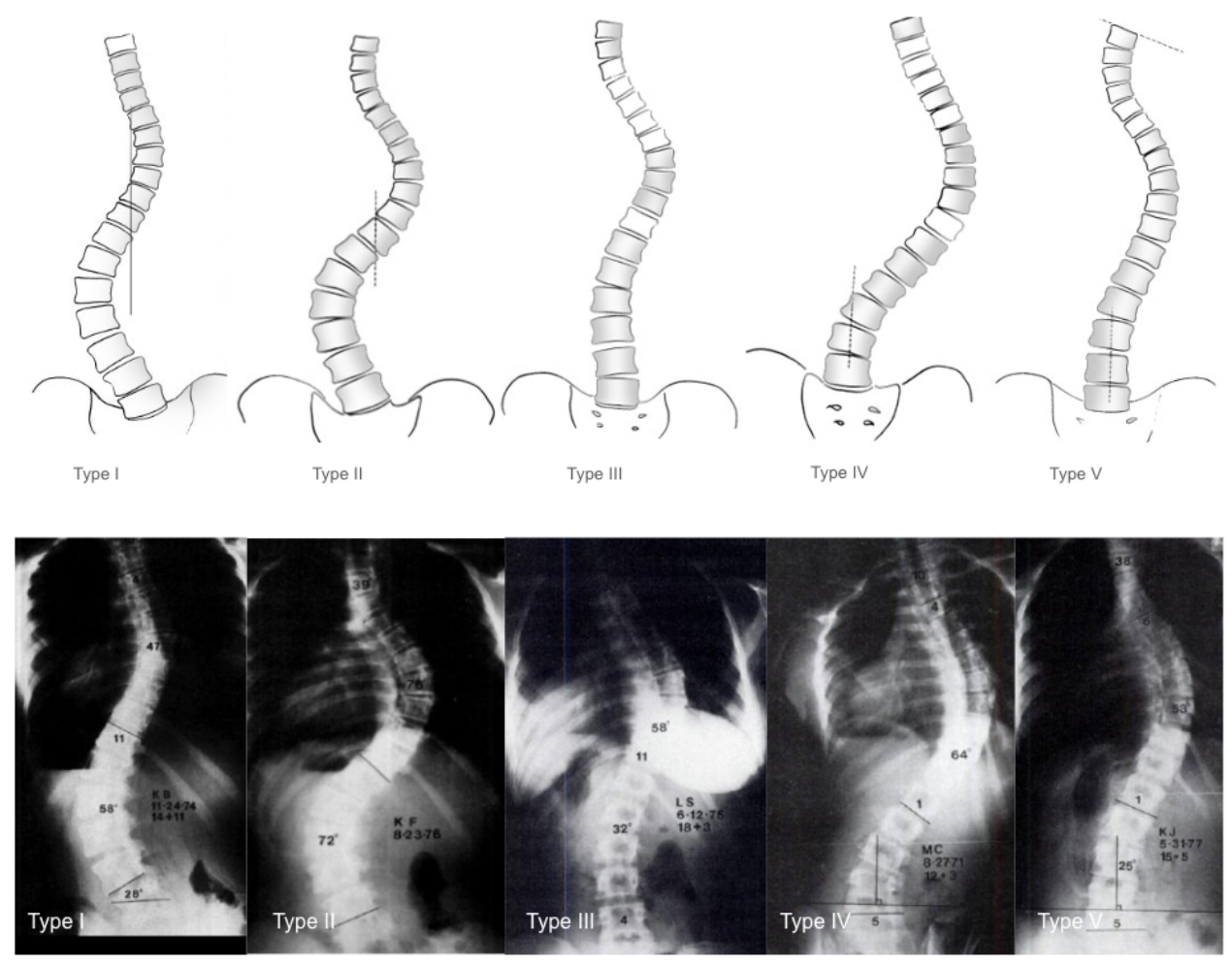
Type I: S-shaped (double curve) with both lumbar and thoracic curves crossing midline; lumbar curve generally larger and stiffer than thoracic curve; FI is generally negative (thoracic curve ≥ lumbar curve standing and more flexible with side-bending)
Type II: S-shaped (double curve) with both lumbar and thoracic curves crossing midline; thoracic curve generally larger and stiffer than lumbar curve; FI generally positive
Type III: Prominent thoracic curve with minimal lumbar compensation (does not cross midline); thoracic ‘overhang’
Type IV: Long thoracic curve where L5 is positioned over sacrum but L4 tilts into thoracic curve
Type V: Double thoracic curve with T1 tilting into apex of upper curve; upper curve appears structural on side-bending
4) Important References
King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am. 1983 Dec;65(9):1302-13.
Smith JS, Shaffrey CI, Kuntz C 4th, Mummaneni PV. Classification systems for adolescent and adult scoliosis. Neurosurgery. 2008 Sep;63(3 Suppl):16-24. doi: 10.1227/01.NEU.0000320447.61835.EA.
Ritzman TF, Floccari LV. The Sagittal Plane in Spinal Fusion for Adolescent Idiopathic Scoliosis. J Am Acad Orthop Surg. 2022 Jul 15;30(14):e957-e967. doi: 10.5435/JAAOS-D-21-01060.
5) Other info....
Historical Role
Designed specifically to guide Harrington rod fusion levels.
Emphasized avoidance of postoperative coronal decompensation.
Key Limitations
Poor inter-observer reliability — different surgeons frequently assigned different curve types.
No sagittal plane assessment — does not account for thoracic kyphosis or lumbar lordosis.
No evaluation of curve flexibility.
Inadequate for modern segmental instrumentation strategies.
Modern Relevance
The King–Moe system has been largely replaced by the Lenke Classification, which incorporates:
Coronal pattern
Sagittal alignment
Curve flexibility
Lenke Classification
Figures adapted from: Lenke LG, Betz RR, Harms J, Bridwell KH, Clements DH, Lowe TG, Blanke K. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am. 2001 Aug;83(8):1169-81.
1) Description of Measurement
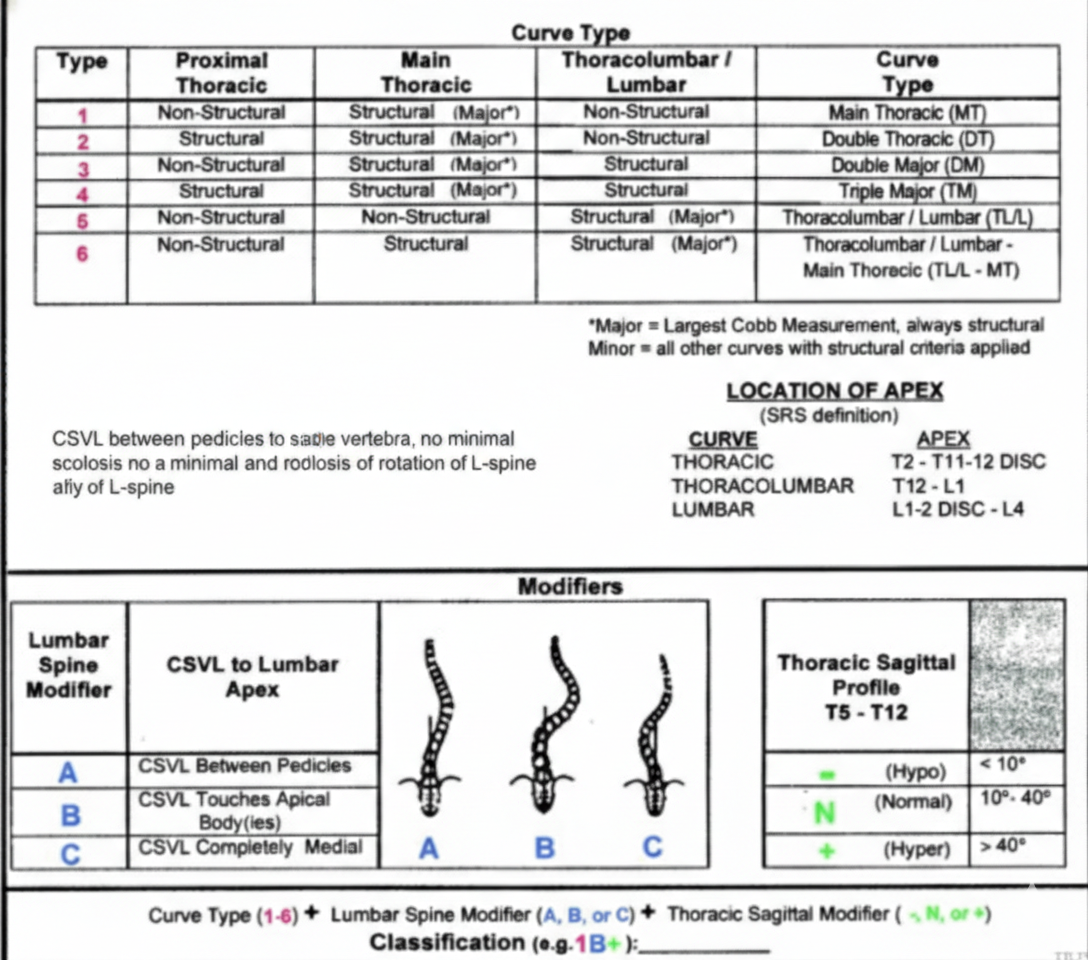
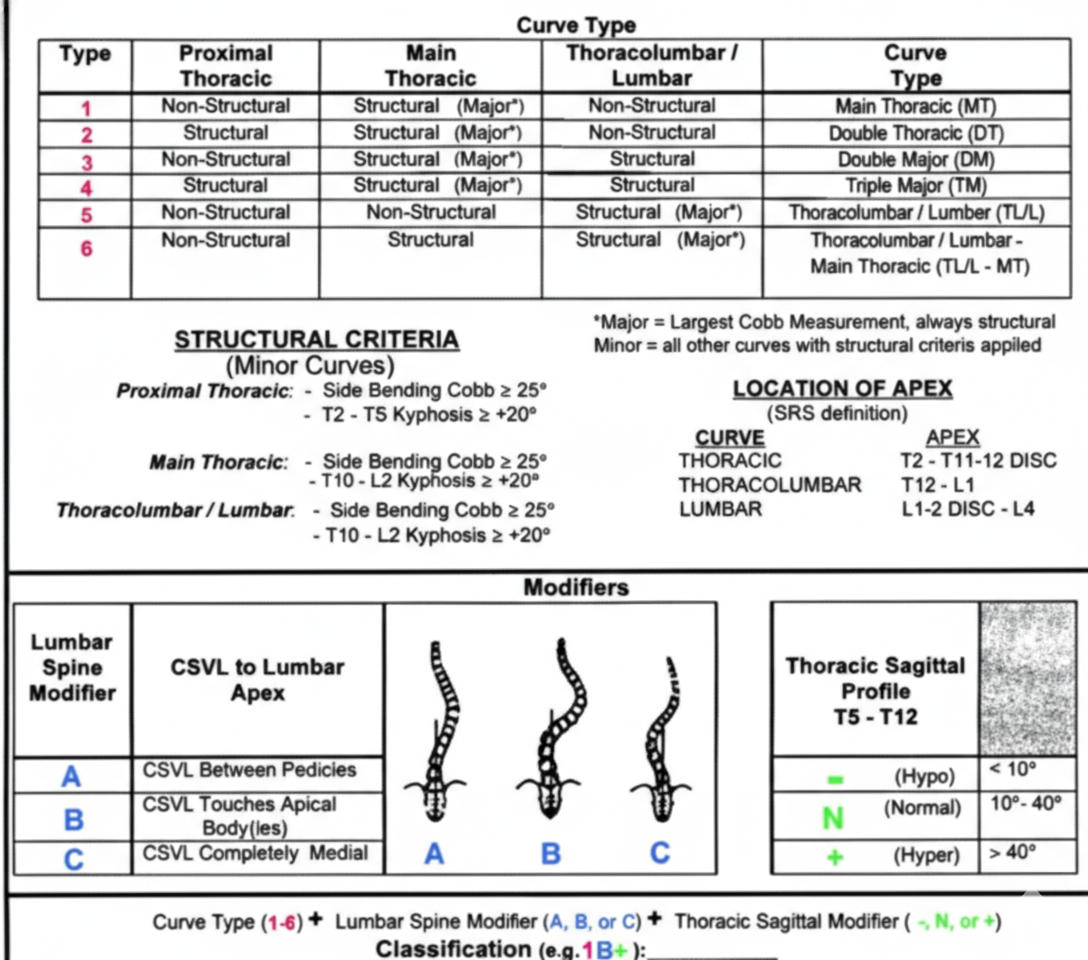
The Lenke Classification System is the contemporary standard for classifying adolescent idiopathic scoliosis (AIS). It defines scoliosis patterns in three dimensions by integrating: (1) Coronal curve type (1-6) to identify the major curve and structural characteristics of the minor curves, (2) Lumbar spine modifier (A, B, C) based on the relationship of the lumbar curve to the central sacral vertical line (CSVL), and (3) Thoracic sagittal modifier (-, N, +) based on its impact on the curvature from T5-T12.
This system distinguishes structural vs non-structural curves, enabling surgeons to determine which curves require inclusion in fusion constructs.
2) Instructions to Measure
Identify curve Type
Obtain four radiographs of the spine (standing long cassette coronal and sagittal, as well as right and left supine bending)
Structural Criteria:
Side bending Cobb angle ≥ 25°, or
Kyphosis
T2-T5 > 20° (proximal thoracic)
T10-L2 > 20° (thoracolumbar/lumbar)
Curve Types:
Type 1: Main thoracic (structural MT)
Type 2: Double thoracic (structural PT and MT)
Type 3: Double major (structural MT and TL/L)
Type 4: Triple major (structural PT, MT*, TL/L*)
Type 5: Thoracolumbar/lumbar (structural TL/L)
Type 6: Thoracolumbar/lumbar-Main thoracic (structural MT and TL/L)
Structural proximal thoracic (PT) curves have Cobb angles of 25° on side-bending xrays and/or kyphosis between T2-T5 of ≥ 20°. Structural main thoracic (MT) curves have Cobb angles of 25° on side-bending xrays and/or kyphosis between T10-L2 of ≥ 20°. Structural thoracolumbar/lumbar (TL) curves have Cobb angles of 25° on side-bending xrays and/or kyphosis between T10-L2 of ≥ 20°. *Either the main thoracic or the thoracolumbar/lumbar curve can be the major curve.
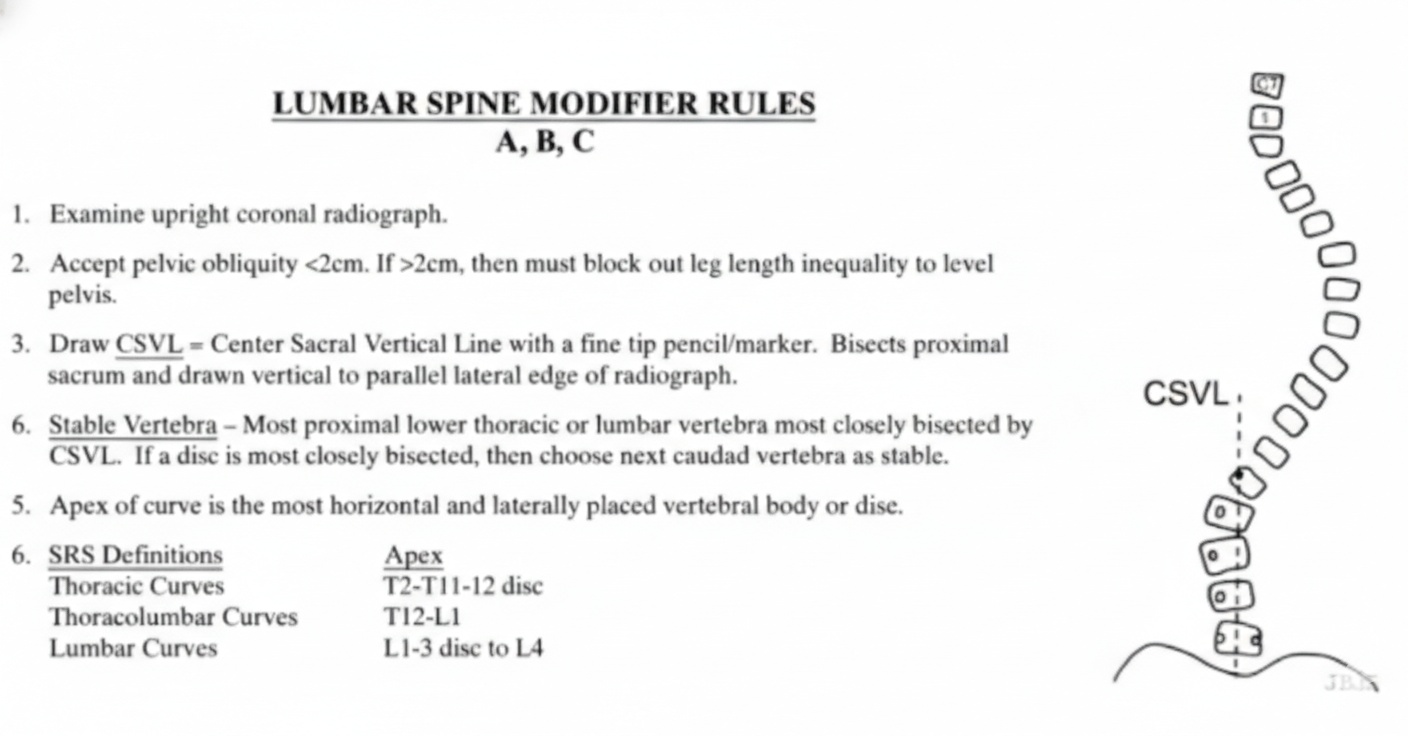
Assign Lumbar Modifier (A, B, C), Draw Central Sacral Vertical Line (CSVL)
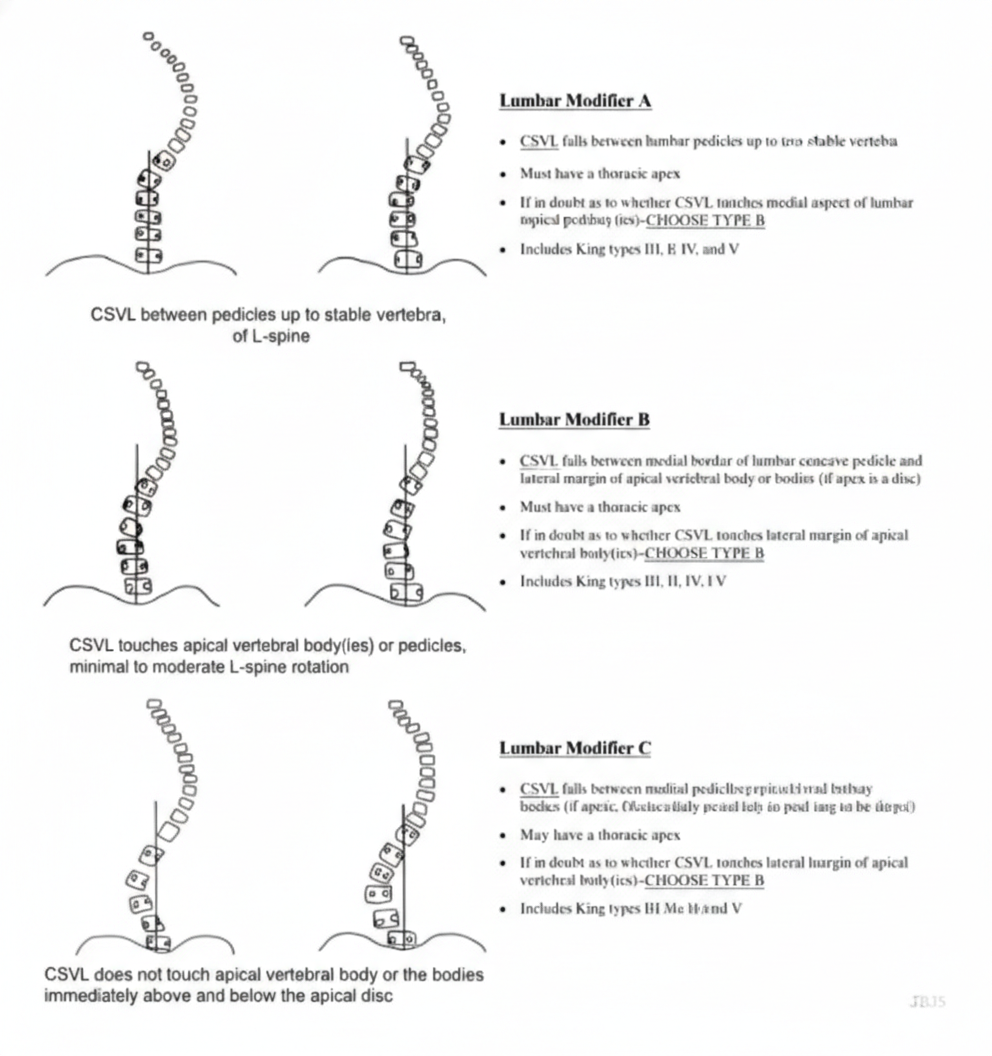
A: CSVL passes between pedicles of stable/apical lumbar vertebra; thoracic apex; no/minimal scoliosis/rotation of lumbar spine (Types 1-4 only)
B: CSVL touches lumbar apical body; thoracic apex; minimal/moderate rotation of lumbar spine
C: CSVL medial to apical lumbar vertebra; main thoracic (Types 1-4), thoracolumbar, and/or lumbar apex (Types 5 and 6)
2. Assign Thoracic Sagittal Modifier, Measures T5-T12 kyphosis on lateral radiograph
(-): < 10° (hypokyphosis)
N: 10° - 40° (normal kyphosis)
(+): > 40° (hyperkyphosis)
3) Normal vs. Pathologic Ranges
Normal Side-bending Cobb: < 25°
Pathologic Side-bending Cobb: ≥ 25°; (structural deformity)
Normal T5-T12 Kyphosis: 10 - 40°
Hypo-/Hyperkyphosis: < 10° (-), >40 (+)
CSVL relative to Lumbar Apex (Normal): Between Pedicles (A)
CSVL relative to Lumbar Apex (Pathologic): Touching/medial to pedicles (B/C)
4) Important References
Lenke L, Betz R, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001; 83A: 1169–81.
Richards BS, Sucato DJ, Konigsberg DE, Ouellet JA. Comparison of reliability between the Lenke and King classification systems for adolescent idiopathic scoliosis using radiographs that were not premeasured. Spine (Phila Pa 1976). 2003 Jun 1;28(11):1148-56; discussion 1156-7. doi: 10.1097/01.BRS.0000067265.52473.C3.
Puno RM, An KC, Puno RL, Jacob A, Chung SS. Treatment recommendations for idiopathic scoliosis: an assessment of the Lenke classification. Spine (Phila Pa 1976). 2003 Sep 15;28(18):2102-14; discussion 2114-5. doi: 10.1097/01.BRS.0000088480.08179.35.
Lenke LG, Edwards CC 2nd, Bridwell KH. The Lenke classification of adolescent idiopathic scoliosis: how it organizes curve patterns as a template to perform selective fusions of the spine. Spine (Phila Pa 1976). 2003 Oct 15;28(20):S199-207. doi: 10.1097/01.BRS.0000092216.16155.33.
5) Other info....
The Lenke system determines fusion strategy:
Structural curves must be fused.
Non-structural curves may be spared to preserve motion.
It improved outcomes over King–Moe by:
Including sagittal alignment
Improving inter-observer reliability
Reducing postoperative coronal decompensation
SRS–Schwab Classification (2012)
1) Description of Measurement
The SRS–Schwab ASD Classification (2012) classifies adult spinal deformity (ASD) based on radiographic parameters linked to pain, disability, and HRQOL. It improves earlier systems by including sagittal alignment and the spine-pelvis interaction. The system has two components.
Coronal curve type describes the location and magnitude of scoliosis, and
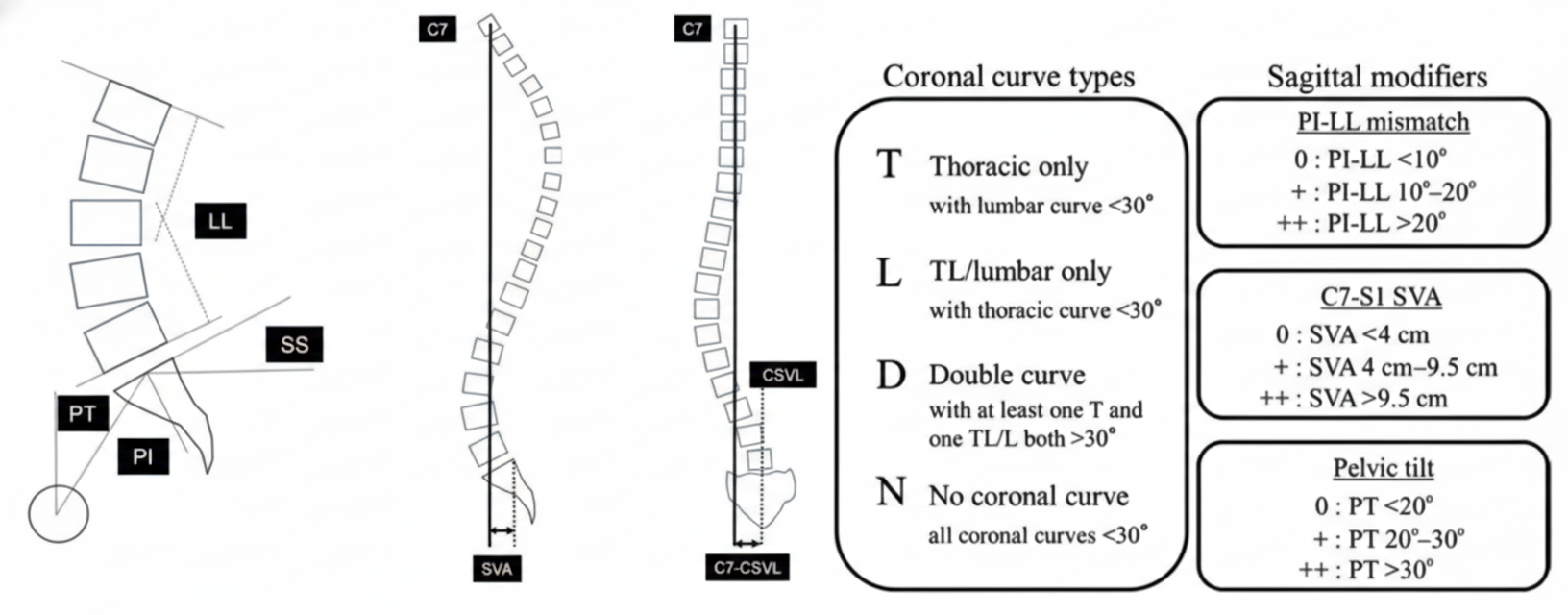
Sagittal modifiers quantify global balance and pelvic compensation using PI–LL mismatch, sagittal vertical axis (SVA), and pelvic tilt (PT). These modifiers capture both the severity of the deformity and the compensatory mechanisms patients use to remain upright.
2) Instructions to Measure
Imaging requirements: standing full-length AP and lateral radiographs, including C7 and both femoral heads.
A) Coronal curve type (PA radiograph)
Measure Cobb angles of thoracic and lumbar curves.
Only curves >30° are considered.
T (thoracic major): thoracic curve >30°, apex at T9 or cranial
L (lumbar major): thoracolumbar/lumbar curve >30°, apex at T10 or caudal
D (double major): both thoracic and lumbar curves >30°
N (normal): no coronal curve >30°
B) Sagittal modifiers (lateral radiograph)
Pelvic Incidence (PI)
Angle between a line perpendicular to the S1 endplate at its midpoint and a line connecting that point to the femoral head axis.
Fixed morphologic parameter.
Lumbar Lordosis (LL)
Cobb angle from L1 superior endplate to S1 superior endplate.
PI–LL mismatch
Calculated as PI minus LL; reflects harmony between pelvic morphology and lumbar curvature.
SVA
Horizontal distance between the C7 plumb line and the posterosuperior corner of S1.
PT
Angle between the vertical and the line connecting the midpoint of the S1 endplate to the femoral head axis.
Reflects pelvic retroversion, a key compensatory mechanism.
3) Normal vs. Pathologic Ranges
Each sagittal modifier is graded by severity.
PI–LL mismatch
0: <10°
+ (1): 10–20°
++ (2): >20°
SVA
0: <40 mm
+ (1): 40–95 mm
++ (2): >95 mm
PT
0: <20°
+ (1): 20–30°
++ (2): >30°
Thresholds associated with severe disability (ODI >40) include:
PT >22°
PI–LL >11°
SVA >46 mm
4) Important References
Terran J, Schwab F, Shaffrey CI, Smith JS, Devos P, Ames CP, Fu KM, Burton D, Hostin R, Klineberg E, Gupta M, Deviren V, Mundis G, Hart R, Bess S, Lafage V; International Spine Study Group. The SRS-Schwab adult spinal deformity classification: assessment and clinical correlations based on a prospective operative and nonoperative cohort. Neurosurgery. 2013 Oct;73(4):559-68. doi: 10.1227/NEU.0000000000000012. PMID: 23756751.
Lowe T, Berven SH, Schwab FJ, Bridwell KH. The SRS classification for adult spinal deformity: building on the King/Moe and Lenke classification systems. Spine (Phila Pa 1976). 2006 Sep 1;31(19 Suppl):S119-25. doi: 10.1097/01.brs.0000232709.48446.be. PMID: 16946628.
Bess S, Schwab F, Lafage V, Shaffrey CI, Ames CP. Classifications for adult spinal deformity and use of the Scoliosis Research Society-Schwab Adult Spinal Deformity Classification. Neurosurg Clin N Am. 2013 Apr;24(2):185-93. doi: 10.1016/j.nec.2012.12.008. PMID: 23561557.
Diebo BG, Varghese JJ, Lafage R, Schwab FJ, Lafage V. Sagittal alignment of the spine: What do you need to know? Clin Neurol Neurosurg. 2015 Dec;139:295-301. doi: 10.1016/j.clineuro.2015.10.024. Epub 2015 Oct 28. PMID: 26562194.
5) Other info....
Age-adjusted modifications (Lafage et al. 2022) have been proposed to account for age-related changes in alignment targets.