
Bone Quality & Bone Mineral Density (BMD)
Hounsfield Units (HU)
1) Description of Measurement
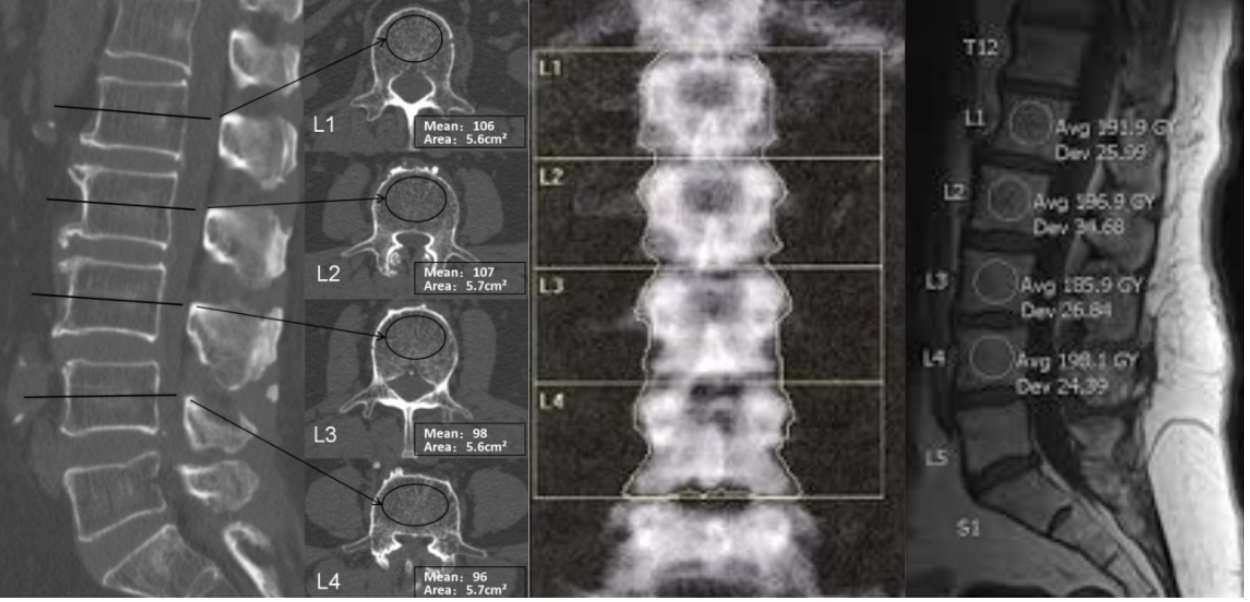
Hounsfield Units (HU) are a standardized, dimensionless measure of X-ray attenuation on CT, derived from the linear attenuation coefficient (μ) of a voxel relative to water: HU = 1000 × (μ_voxel − μ_water)/(μ_water − μ_air), with water defined as 0 HU and air as −1,000 HU. HU denotes the gray-scale value of each pixel, based on the extent to which the tissue attenuates the X-ray beam relative to water. Within the vertebral body, HU reflects trabecular bone, marrow fat, and, in some cases, cortical shell attenuation. Because trabecular bone is the metabolically active compartment most sensitive to osteoporotic change, trabecular HU within the cancellous centrum serves as an “opportunistic” surrogate for bone mineral density (BMD). Studies show strong links between lumbar HU, DXA BMD/T scores, and mechanical strength, supporting HU as a practical CT-based bone quality measure when DXA is unavailable or unclear.
2) Instructions to Measure
Prefer noncontrast CT (slice thickness ≤3 mm). If contrast-enhanced CT is used, record phase (arterial/venous/delayed) and contrast status as covariates, as attenuation can increase modestly with enhancement.
HU values are automatically calculated during CT reconstruction using tissue attenuation coefficients. Gray-scale values result from filtered back projection, converting X-ray measurements into CT numbers.
ROI placement (trabecular centrum technique):
Use axial images, preferably, and select the mid vertebral body region (about mid-height between endplates) to minimize partial volume effects from endplates and osteophytes.
Acquire HU from 3 consecutive axial slices centered at mid-body (or the closest available) and average the mean HU across slices.
Place a large elliptical or circular ROI within the cancellous bone, centered in the vertebral body, targeting trabecular tissue.
Avoid cortical bone by keeping a margin from the anterior, lateral, and posterior cortical shells (do not contact the cortex).
Exclude surrounding tissues, different from the vertebral body, and hardware artifacts.
3) Normal vs. Pathologic Ranges
Because HU is scanner-dependent and continuous, thresholds serve as decision-support tools, not definitive diagnostic criteria. Typical opportunistic screening thresholds based on L1 trabecular attenuation are:
Normal / low osteoporosis risk: >160 HU (high sensitivity).
Osteopenia risk: 100–160 HU (consider DXA).
Likely osteoporosis: <100 HU (high specificity).
4) Important References
Schreiber JJ, Anderson PA, Rosas HG, Buchholz AL, Au AG. Hounsfield units for assessing bone mineral density and strength: a tool for osteoporosis management. J Bone Joint Surg Am. 2011 Jun 1;93(11):1057-63. doi: 10.2106/JBJS.J.00160. PMID: 21655899.
Pickhardt PJ, Pooler BD, Lauder T, del Rio AM, Bruce RJ, Binkley N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann Intern Med. 2013 Apr 16;158(8):588-95. doi: 10.7326/0003-4819-158-8-201304160-00003. PMID: 23588747; PMCID: PMC3736840.
Emohare O, Cagan A, Morgan R, Davis R, Asis M, Switzer J, Polly DW Jr. The use of computed tomography attenuation to evaluate osteoporosis following acute fractures of the thoracic and lumbar vertebra. Geriatr Orthop Surg Rehabil. 2014 Jun;5(2):50-5. doi: 10.1177/2151458514525042. PMID: 25360331; PMCID: PMC4212365.
5) Other info....
HU is not a calibrated densitometry measurement. Variation in kVp, reconstruction kernel, iterative reconstruction, and scanner model can meaningfully shift HU.
DEXA Scan
Adapted from: Non-contrast-enhanced T1-weighted MRI of the lumbar spine demonstrating regions of interest used to calculate the L1–L4 vertebral body quality (VBQ) score, Journal of Clinical Medicine (Accessed on 03 Jan 2026).
1) Description of Measurement
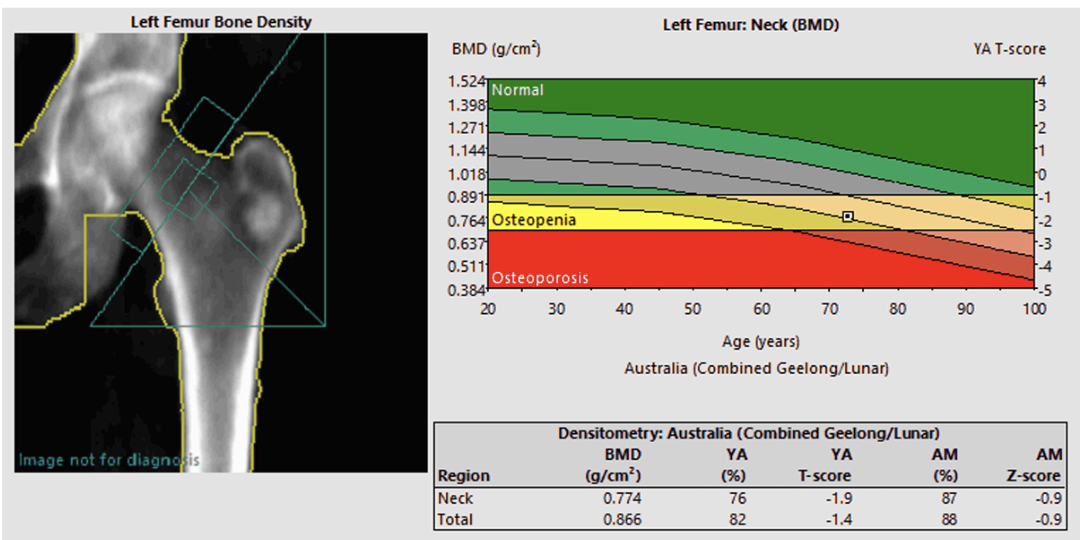
Dual-energy X-ray absorptiometry (DXA or DEXA) quantifies areal bone mineral density (aBMD) in g/cm² at standardized skeletal regions of interest. It is a low-dose X-ray technique that measures bone mineral density BMD using two energy X-rays to determine calcium and mineral levels. The differential attenuation of X-ray beams enables calculation of bone mineral content and soft-tissue attenuation within the scan region. DEXA provides absolute aBMD and standardized scores:
T-score: number of standard deviations from young-adult reference mean. This is the main metric for diagnosing osteoporosis in postmenopausal women and men ≥50, and it anchors most treatment thresholds.
Z-score indicates deviations from age-, sex-, and ancestry-matched means, especially useful in premenopausal women, men <50, and secondary osteoporosis. A low Z-score (often ≤ −2.0) suggests “below the expected range for age” and warrants further workup, not a T-score diagnosis.
2) Instructions to Measure
DEXA examinations are typically performed at the lumbar spine (L1-L4), hip (including femoral neck, greater trochanter, and total hip), or forearm. Proper patient positioning and scan analysis are critical because positioning errors or artifacts (such as osteoarthritis, fractures, or jewelry) can compromise accuracy.
Select the diagnostic hip value by using either the femoral neck or total hip (whichever yields the lower measurement) for classification; measurement can be taken on either hip. PA lumbar aBMD may be artificially increased due to factors such as degenerative facet arthropathy and osteophytes, endplate sclerosis, vertebral compression fractures, significant scoliosis or rotation, prior fusion, instrumentation, cement augmentation, or other hardware. If the central sites are inaccessible—due to bilateral hip hardware, extensive lumbar instrumentation or arthrodesis, severe deformity, or rotation—then obtain forearm DEXA.
3) Normal vs. Pathologic Ranges
According to World Health Organization criteria:
Normal: T-score ≥ -1.0
Low bone mass (osteopenia): -1.0 and -2.5
Osteoporosis: T-score ≤ -2.5
4) Important References
Jain RK, Vokes T. Dual-energy X-ray Absorptiometry. J Clin Densitom. 2017 Jul-Sep;20(3):291-303. doi: 10.1016/j.jocd.2017.06.014. Epub 2017 Jul 14. PMID: 28716497.
LeBoff MS, Greenspan SL, Insogna KL, Lewiecki EM, Saag KG, Singer AJ, Siris ES. The clinician's guide to prevention and treatment of osteoporosis. Osteoporos Int. 2022 Oct;33(10):2049-2102. doi: 10.1007/s00198-021-05900-y. Epub 2022 Apr 28. Erratum in: Osteoporos Int. 2022 Oct;33(10):2243. doi: 10.1007/s00198-022-06479-8. PMID: 35478046; PMCID: PMC9546973.
El Maghraoui A, Roux C. DXA scanning in clinical practice. QJM. 2008 Aug;101(8):605-17. doi: 10.1093/qjmed/hcn022. Epub 2008 Mar 10. PMID: 18334497.
Sardar ZM, Coury JR, Cerpa M, DeWald CJ, Ames CP, Shuhart C, Watkins C, Polly DW, Dirschl DR, Klineberg EO, Dimar JR, Krohn KD, Kebaish KM, Tosi LL, Kelly M, Lane NE, Binkley NC, Berven SH, Lee NJ, Anderson P, Angevine PD, Lehman RA, Lenke LG. Best Practice Guidelines for Assessment and Management of Osteoporosis in Adult Patients Undergoing Elective Spinal Reconstruction. Spine (Phila Pa 1976). 2022 Jan 15;47(2):128-135. doi: 10.1097/BRS.0000000000004268. Erratum in: Spine (Phila Pa 1976). 2022 Sep 1;47(17):E581. doi: 10.1097/BRS.0000000000004450. PMID: 34690329.
Lechtholz-Zey EA, Gettleman BS, Ayad M, Mills ES, Shelby H, Ton A, Shah I, Safaee MM, Wang JC, Alluri RK, Hah RJ. The Effect of Osteoporosis on Complications and Reoperation Rates After Surgical Management of Adult Thoracolumbar Spinal Deformity: A Systematic Review and Meta Analysis. Global Spine J. 2024 Nov;14(8):2420-2439. doi: 10.1177/21925682241250031. Epub 2024 Apr 26. PMID: 38666610; PMCID: PMC11528736.
5) Other info....
For each SD decline in BMD, fracture risk increases by 1.5-2.5, showing DEXA's predictive value. However, about half of fragility fractures happen in patients with osteopenia, indicating BMD alone doesn't fully predict fracture risk.
Vertebral Bone Quality (VBQ) Score
Adapted from: Non-contrast-enhanced T1-weighted MRI of the lumbar spine demonstrating regions of interest used to calculate the L1–L4 vertebral body quality (VBQ) score, Journal of Clinical Medicine (Accessed on 03 Jan 2026).
1) Description of Measurement
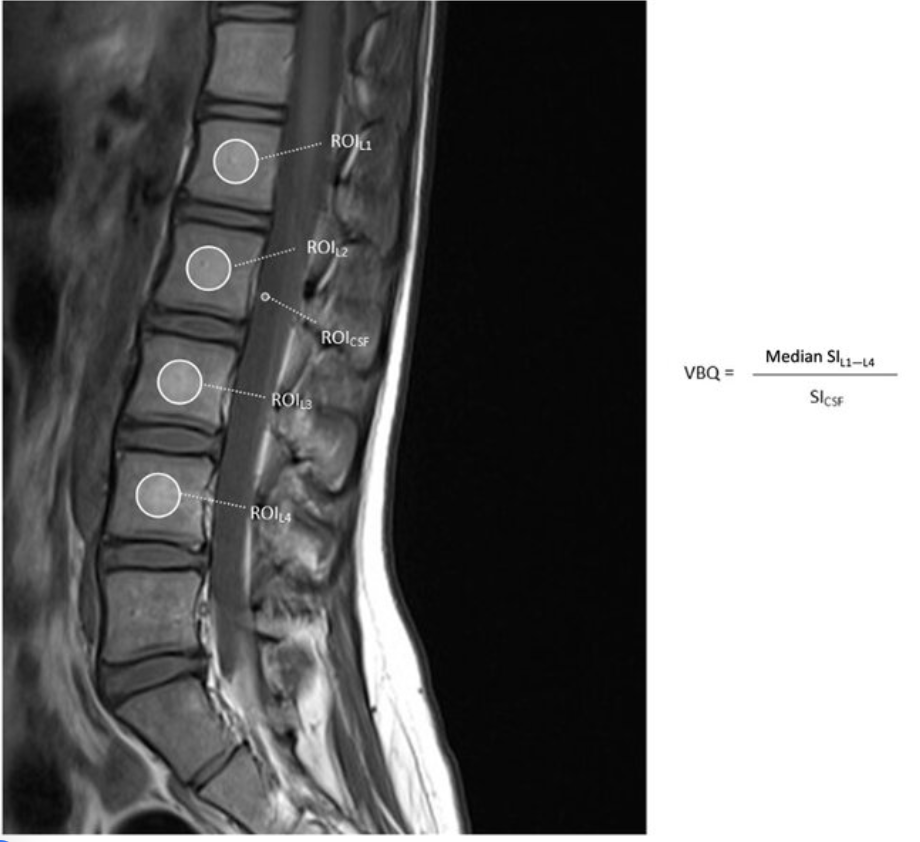
The Vertebral Bone Quality (VBQ) score is an MRI-based measure that quantifies vertebral bone marrow signal intensity to assess bone quality. It serves as an opportunistic screening tool for osteoporosis and bone quality assessment in patients undergoing spine imaging. The VBQ score reflects bone marrow composition, with higher scores indicating increased fat content in the marrow (which correlates with decreased bone quality). The score is calculated as a ratio of vertebral body signal intensity to cerebrospinal fluid (CSF) signal intensity on non-contrast T1-weighted MRI sequences.
2) Instructions to Measure
Obtain midsagittal T1-weighted MRI images of the lumbar spine
Place regions of interest (ROI) within the trabecular bone of L1-L4 vertebral bodies to measure median signal intensity
A separate region of interest is placed within the cerebrospinal fluid (CSF) at the level of the conus or cauda equina to serve as an internal reference. Measure the signal intensity of CSF, typically at the L2 or L3 level (both are comparable)
Calculate VBQ score = (median signal intensity of L1-L4 vertebrae) / (signal intensity of CSF), producing a normalized ratio that can be compared across patients and scanners.
3) Normal vs. Pathologic Ranges
Normal bone quality: VBQ scores typically range from 2.2 to 2.8
Osteopenia/osteoporosis: VBQ scores are significantly elevated, typically ≥3.0 to 3.4
Diagnostic thresholds vary by study and reference standard:
For osteoporosis screening: VBQ >2.95-3.06 suggests need for further evaluation
For predicting fragility fractures: ≥3.05 indicates increased risk
4) Important References
Salzmann SN, Okano I, Jones C, Zhu J, Lu S, Onyekwere I, Balaji V, Reisener MJ, Chiapparelli E, Shue J, Carrino JA, Girardi FP, Cammisa FP, Sama AA, Hughes AP. Preoperative MRI-based vertebral bone quality (VBQ) score assessment in patients undergoing lumbar spinal fusion. Spine J. 2022 Aug;22(8):1301-1308. doi: 10.1016/j.spinee.2022.03.006. Epub 2022 Mar 24. PMID: 35342015.
Zhou Z, Wang JQ, Daniel Mwesigwa K, Chen Y, Jin PL, Dong XY, Zhang HQ, Zhou LP, Jia CY, Kang L, Ma HY, Shen CL, Zhang RJ. Vertebral bone quality score as a novel tool for bone mineral density assessment: which measurement approach is more accurate? Eur Spine J. 2025 Nov 10. doi: 10.1007/s00586-025-09544-y. Epub ahead of print. PMID: 41207959.
Zhou Z, Wang JQ, Daniel Mwesigwa K, Chen Y, Jin PL, Dong XY, Zhang HQ, Zhou LP, Jia CY, Kang L, Ma HY, Shen CL, Zhang RJ. Vertebral bone quality score as a novel tool for bone mineral density assessment: which measurement approach is more accurate? Eur Spine J. 2025 Nov 10. doi: 10.1007/s00586-025-09544-y. Epub ahead of print. PMID: 41207959.
Kim AYE, Lyons K, Sarmiento M, Lafage V, Iyer S. MRI-Based Score for Assessment of Bone Mineral Density in Operative Spine Patients. Spine (Phila Pa 1976). 2023 Jan 15;48(2):107-112. doi: 10.1097/BRS.0000000000004509. Epub 2022 Oct 17. PMID: 36255388.
5) Other info....
Unlike DXA, which provides areal bone density, the VBQ score assesses microstructural bone quality and correlates more strongly with osteoporosis, fracture risk, and surgical complications. While it shows a moderate-to-strong correlation with DXA T-scores, particularly in older adults, it should be used for risk stratification rather than as a standalone diagnostic.