
Image Type
Facet Join Orientation and Tropism
1) Description of Measurement
Facet joint orientation describes the angular relationship of the lumbar zygapophyseal joints relative to the midsagittal plane. Orientation reflects biomechanical behavior of the motion segment:
Smaller axial angles → sagittalized facets
Larger axial angles → coronally oriented facets
Facet tropism represents asymmetry between right and left facet joint angles, causing uneven motion and asymmetric load transfer. According to the attached study, facet tropism is defined as a bilateral difference > 10° in the axial plane. A smaller angle indicates sagittal orientation, while a larger angle indicates coronal orientation.
2) Instructions to Measure
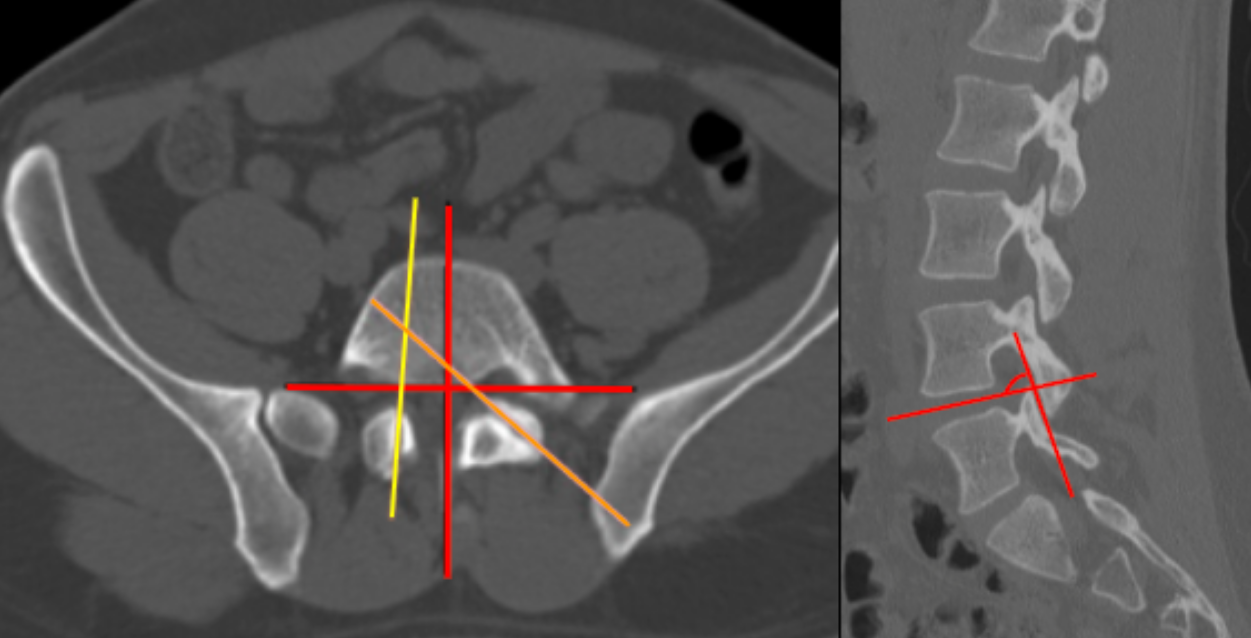
Select the axial CT slice that bisects the intervertebral disc at the level of interest.
For each facet joint:
Draw a facet line connecting the anteromedial and posterolateral edges of the articular surface.
Draw a midsagittal reference line perpendicular to the posterior vertebral body wall through the base of the spinous process.
Measure the facet joint angle between the facet line and the midsagittal reference line for:
Right facet
Left facet
Calculate:
Mean facet orientation = average of left and right angles.
Facet tropism = absolute difference between left and right facet angles.
Select the parasagittal CT slice that shows the facet joint of interest
For each facet joint:
Draw a line between the anterosuperior edge and posteroinferior edge of each facet joint
Draw another line which bisects the intervertebral disc of the corresponding level
Measure the facet joint angle between the facet line and the intervertebral disc line
Calculate:
Mean facet orientation = average of left and right angles.
Facet tropism = absolute difference between left and right facet angles.
3) Normal vs. Pathologic Ranges
Sagittal orientation (sagittalization): Small axial angle
Coronal orientation (coronalization): Large axial angle
Normal symmetry: Left-right difference ≤ 10°
Facet tropism (pathologic): Left-right difference > 10°
4) Important References
Ishihama Y, Tezuka F, Manabe H, et al. Facet Joint Morphology and Tropism in Adolescents: Association With Lumbar Disk Herniation and Spondylolysis. Spine (Phila Pa 1976). 2024 Jul 15;49(14):1029-1035. doi: 10.1097/BRS.0000000000004818.
Ranjbar E, Alizadeh SD, Mirkamali H, et al. Facet joint tropism in degenerative lumbar scoliosis: a retrospective case-control study. Spine Deform. 2025 May;13(3):897-902. doi: 10.1007/s43390-024-01037-0.
Carneiro VM, Pongeluppi RI, Fernandes DS, et al. Correlations Between Facet Tropism, Joint Mobility and Degree of Displacement in Patients with Low Grade Spondylolisthesis. Turk Neurosurg. 2024;34(6):1050-1055. doi: 10.5137/1019-5149.JTN.40720-22.3.
5) Other info....
Axial facet tropism is particularly prevalent at L4–5 and is associated with lumbar disc herniation and spondylolysis, especially in adolescents.
Coronalized facets increase rotational stress, while sagittalized facets predispose to shear-related pathologies.
Adapted from: Weerakkody Y, Skandhan A, Luong D, et al. Facet joint tropism. Reference article, Radiopaedia.org (Accessed on 04 Jan 2026) https://doi.org/10.53347/rID-90699