
Image Type
Vertebral Body Dimensions
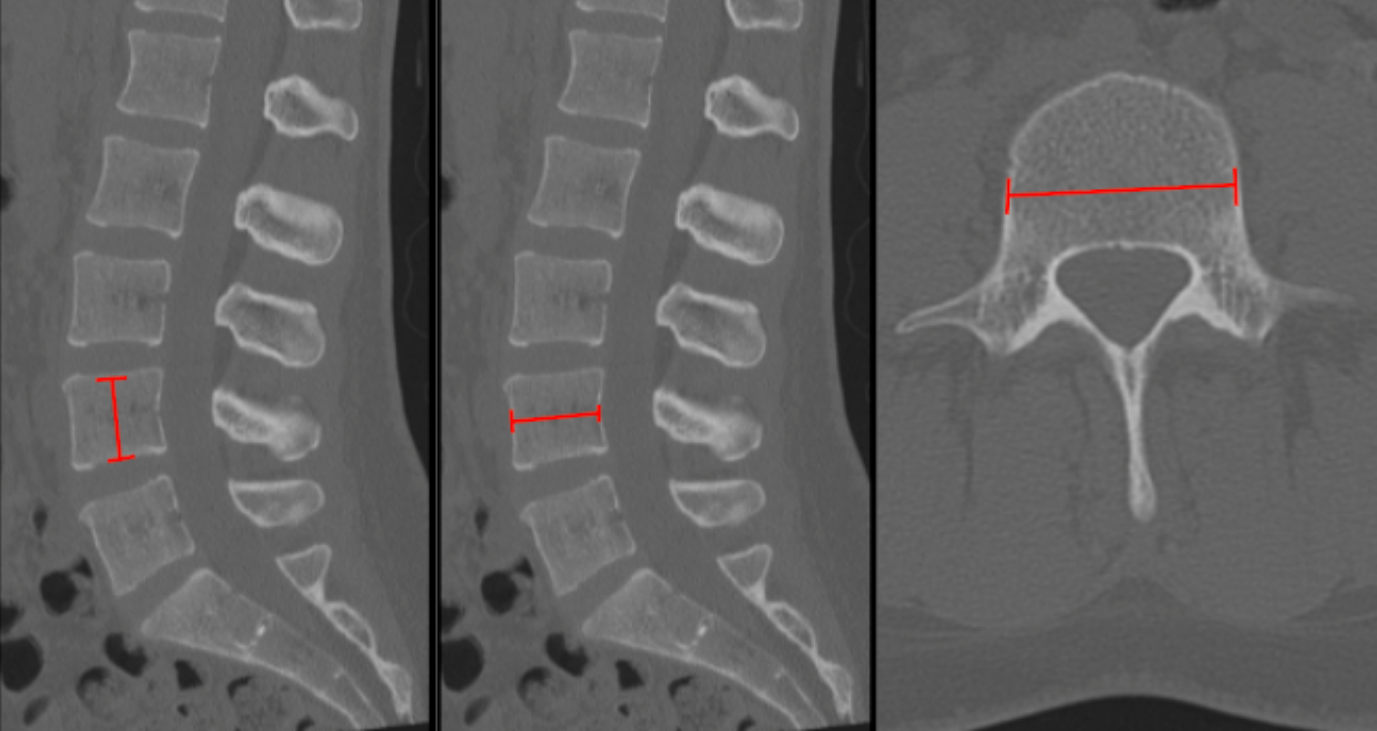
1) Description of Measurement
Vertebral body dimensions quantify the size and morphology of each lumbar vertebral body. These measurements are essential for:
Identifying compression fractures or vertebral wedging
Assessing degenerative collapse
Preoperative planning for interbody devices, cages, and instrumentation
Evaluating congenital hypoplasia or remodeling from deformity or trauma
Dimensions include:
Vertebral Body Height (superior–inferior)
Anteroposterior (AP) Depth
Transverse Width (mediolateral diameter)
2) Instructions to Measure
Step 1 – Select Proper Slice
Use thin-slice (≤1 mm) sagittal and axial CT reconstructions.
Ensure the slice passes through the mid-vertebral body (avoid pedicles/endplates).
Step 2 – Vertebral Body Height (Sagittal CT)
On a true mid-sagittal image:
Measure from the midpoint of the superior endplate to the midpoint of the inferior endplate.
If wedged, measure anterior, middle, and posterior heights and record the minimum.
Step 3 – AP Depth (Axial or Sagittal CT)
On Sagittal CT through the mid-vertebral body:
Measure from the anterior cortex to posterior cortex at the midline of the vertebral body.
Step 4 – Transverse Width (Axial CT)
On the same axial slice:
Measure the maximum mediolateral diameter of the vertebral body between the lateral cortical margins.
Step 5 – Documentation
Record dimensions in millimeters (mm) for each lumbar level.
Compare adjacent levels and contralateral symmetry when applicable.
3) Normal vs. Pathologic Ranges
Vertebral Body Height
Normal: 20-30 mm
Pathologic: < 20 mm or > 20% loss vs adjacent = compression fracture
AP Depth
Normal: 30-35 mm (L3-L5)
Pathologic: reduced in collapse; enlarged with remodeling or deformity
Transverse Width
Normal: 40-50 mm
Pathologic: Marked asymmetry or focal loss suggests fracture or lytic process
Height Ratio (Anterior/Posterior)
Normal 1.0
Pathologic: < 0.8 indicates wedge fracture
4) Important References
Ferrar L, Jiang G, Adams J, Eastell R. Identification of vertebral fractures: an update. Osteoporos Int. 2005 Jul;16(7):717-28. doi: 10.1007/s00198-005-1880-x. Epub 2005 May 3.
Vaccaro AR, Oner C, Kepler CK, et al; AOSpine Spinal Cord Injury & Trauma Knowledge Forum. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine (Phila Pa 1976). 2013 Nov 1;38(23):2028-37. doi: 10.1097/BRS.0b013e3182a8a381.
Schnake KJ, Schroeder GD, Vaccaro AR, Oner C. AOSpine Classification Systems (Subaxial, Thoracolumbar). J Orthop Trauma. 2017 Sep;31 Suppl 4:S14-S23. doi: 10.1097/BOT.0000000000000947.
5) Other info....
Always measure at the true mid-vertebral level to avoid overestimating due to endplate irregularities.
In trauma, compare anterior vs posterior height to detect subtle burst or wedge fractures.
Vertebral body dimensions are critical for selecting appropriate interbody cage height and footprint.
Progressive decrease in height across serial imaging suggests ongoing collapse or instability.
Adapted from: Feger J, Campos A, Murphy A, et al. CT lumbar spine (protocol). Reference article, Radiopaedia.org (Accessed on 03 Jan 2026) https://doi.org/10.53347/rID-90041