
Image Type
Canal Compromise Percentage
1) Description of Measurement
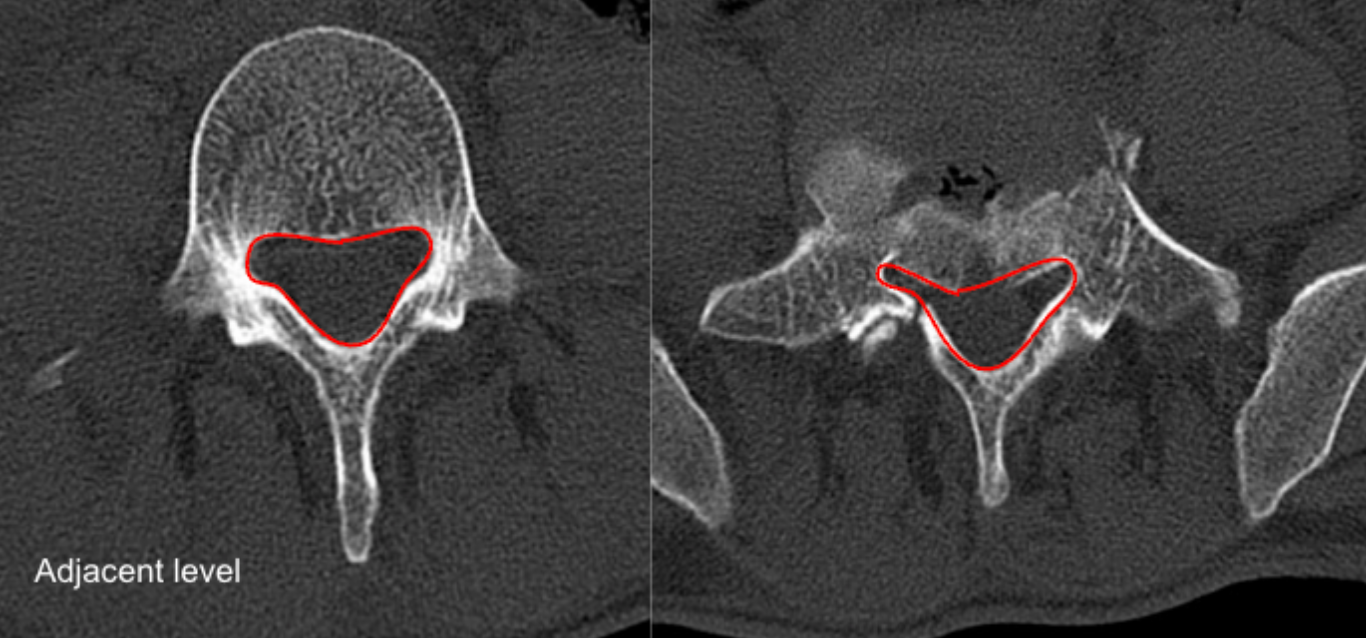
Canal Compromise Percentage estimates the proportion of the normal spinal canal that is occupied by retropulsed bony fragments following burst fracture. It is calculated by comparing the cross-sectional area (CSA) of the normal canal at an adjacent level with the residual canal area at the injured level.
This measurement correlates with neurological risk, severity of canal stenosis, and is often used when determining the need for decompression.
2) Instructions to Measure
Imaging Requirements
Thin-slice axial CT through the fracture level and adjacent intact levels.
Step-by-Step
Select Reference Level (Normal Canal)
Choose the nearest intact level above or below the fracture.
Use axial CT to outline the bony spinal canal.
Measure cross-sectional area → A₀ (Normal Canal Area, mm²).
Select Injured Level
Identify the level with maximal retropulsed fragments.
Trace the remaining free canal lumen excluding bony fragments.
Measure residual canal area → Aᵢ (Injured Canal Area, mm²).
Calculate Canal Compromise %
Canal Compromise (%) = (A0 - Ai)/A0*100
Record
Level measured
A0, Ai, and calculated %
3) Normal vs. Pathologic Ranges
Normal/minimal compromise: 0-10%
Mild compromise: 10-25%
Moderate compromise: 25-40%
Severe compromise (high risk for neurologic injury): > 40%
Critical stenosis (often surgical): > 50%
Clinical correlation with the neurologic exam is mandatory.
4) Important References
Milavec H, Gasser VT, Ruder TD, et al. Supplementary value and diagnostic performance of computed tomography scout view in the detection of thoracolumbar spine injuries. Emerg Radiol. 2024 Feb;31(1):63-71. doi: 10.1007/s10140-023-02196-9.
Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine (Phila Pa 1976). 1983 Nov-Dec;8(8):817-31. doi: 10.1097/00007632-198311000-00003.
Meves R, Avanzi O. Correlation among canal compromise, neurologic deficit, and injury severity in thoracolumbar burst fractures. Spine (Phila Pa 1976). 2006 Aug 15;31(18):2137-41. doi: 10.1097/01.brs.0000231730.34754.9e.
Yuan L, Yang S, Luo Y, et al. Surgical consideration for thoracolumbar burst fractures with spinal canal compromise without neurological deficit. J Orthop Translat. 2019 Dec 30;21:8-12. doi: 10.1016/j.jot.2019.12.003.
5) Other info....
CT is superior to radiographs for canal compromise assessment.
MRI may be added to assess neural compression, ligamentous injury, and cord/cauda equina edema.
Retropulsed fragment size does not always correlate with neurologic deficit; morphology and dynamic factors also matter.
Measurement should be performed at the maximally compromised axial slice, not mid-vertebral level.
Adapted from: Niknejad M, Burst fracture. Case study, Radiopaedia.org (Accessed on 05 Jan 2026) https://doi.org/10.53347/rID-93541