
Image Type
Cross-Sectional Area (CSA) of Spinal Canal
1) Description of Measurement
Lumbar spinal canal cross-sectional area (CSA) quantifies the total area available for the cauda equina within the central canal. It is a sensitive morphologic marker for lumbar spinal stenosis and correlates more closely with symptom severity than single-dimension measurements such as AP canal diameter.
CSA incorporates the combined effects of disc bulge, facet hypertrophy, ligamentum flavum thickening, and spondylolisthesis, providing a global assessment of central canal compromise.
2) Instructions to Measure
Identify the lumbar level of maximal stenosis on sagittal MRI.
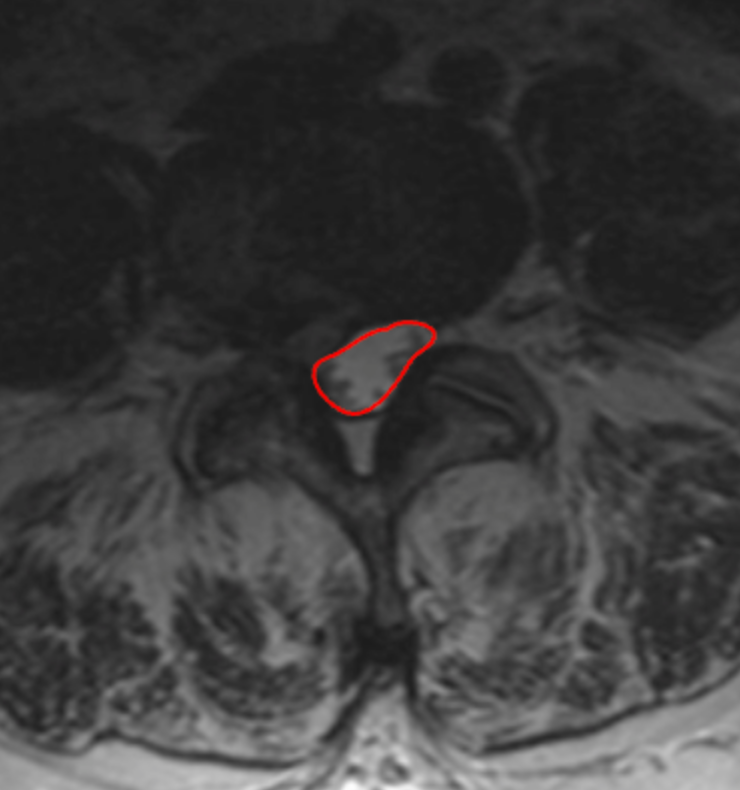
Scroll to the corresponding axial T2 slice at the disc level or mid-vertebral body level.
Using a freehand or polygon ROI tool, trace the inner bony and ligamentous margins of the spinal canal, including thecal sac and excluding osteophytes or epidural fat.
Close the region of interest to generate the cross-sectional area (mm²).
Record the smallest CSA across all lumbar levels.
3) Normal vs. Pathologic Ranges
Normal: > 100 mm2
Relative (moderate) stenosis: 75 - 100 mm2
Severe stenosis: 50 - 75 mm2
Critical stenosis: < 50 mm2
Key points:
Symptomatic neurogenic claudication is most commonly seen when CSA is < 75 mm².
CSA < 50 mm² is strongly associated with severe clinical stenosis.
4) Important References
Abel F, Tan ET, Chazen JL, et al. MRI after Lumbar Spine Decompression and Fusion Surgery: Technical Considerations, Expected Findings, and Complications. Radiology. 2023 Jul;308(1):e222732. doi: 10.1148/radiol.222732.
Hansen BB, Nordberg CL, Hansen P, et al. Weight-bearing MRI of the Lumbar Spine: Spinal Stenosis and Spondylolisthesis. Semin Musculoskelet Radiol. 2019 Dec;23(6):621-633. doi: 10.1055/s-0039-1697937.
Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol. 2010 Apr;24(2):253-65. doi: 10.1016/j.berh.2009.11.001.
5) Other info....
CSA is preferred over AP diameter when:
Compression is asymmetric
There is significant facet hypertrophy or ligamentum flavum infolding
Should be interpreted with:
Lateral recess depth
Foraminal dimensions
Dynamic factors (extension-induced narrowing) are not captured on routine MRI; consider upright or flexion-extension imaging if symptoms and CSA are discordant.
Adapted from: Feger J, Er A, Yap J, et al. Lumbar spine protocol (MRI). Reference article, Radiopaedia.org (Accessed on 01 Jan 2026) https://doi.org/10.53347/rID-147093